12 Digestive System
Topic: Digestive System
Text Reference: Chapter 12. Digestive System
Objectives: Students should be able to…
Identify meanings of key word components of the digestive system
Prefixes
hemi- (half)
endo- (within, in)
sub- (under, below)
dys- (painful, abnormal, difficult, labored)
Combining Forms
abdomin/o (abdomen, abdominal)
an/o (anus)
antr/o (antrum)
append/o (appendix)
appendic/o (appendix)
cec/o (cecum)
celi/o (abdomen, abdominal cavity)
cheil/o (lip)
cholangi/o (bile duct)
chol/e (gall, bile)
choledoch/o (common bile duct)
col/o (colon)
colon/o (colon)
diverticul/o (diverticulum)
duoden/o (duodenum)
enter/o (intestine)
esophag/o (esophagus)
gastr/o (stomach)
gingiv/o (gum)
gloss/o (tongue)
hepat/o (liver)
herni/o (hernia, protrusion of an organ through a membrane or cavity wall)
ile/o (ileum)
jejun/o (jejunum)
lapar/o (abdomen, abdominal cavity)
lingu/o (tongue)
or/o (mouth)
palat/o (palate)
pancreat/o (pancreas)
peritone/o (peritoneum)
polyp/o (polyp, small growth)
proct/o (rectum)
pylor/o (pylorus, pyloric sphincter)
rect/o (rectum)
sial/o (saliva, salivary gland)
sigmoid/o (sigmoid colon)
steat/o (fat)
stomat/o (mouth)
uvul/o (uvula)
Suffixes
-ac (pertaining to)
-al (pertaining to)
-cele (hernia, protrusion)
-centesis (surgical puncture to aspirate fluid)
-ectomy (excision)
-gram (the record, radiographic image)
-graph (instrument used to record)
-graphy (process of recording)
-ia (condition of, diseased state, abnormal state)
-iasis (condition)
-itis (inflammation)
-logist (specialist or physician who studies and treats)
-logy (study of)
-malacia (softening)
-oma (tumor)
-osis (abnormal condition)
-pathy (disease)
-pepsia (digestion)
-phagia (eating or swallowing)
-plasty (surgical repair)
-ptosis (prolapse, drooping)
-rrhaphy (suturing, repairing)
-rrhea (flow, discharge)
-scope (instrument used for visualization)
-scopy (process of viewing, visualization)
-stomy (creation of an artificial opening)
-tomy (incision, cut into)
Apply the rules of medical language to pronounce, break into word parts, and define the following terms.
Label each word part by using the following abbreviations:
P = Prefix
WR = Word Root
CV = Combining Vowel
S = Suffix
CF = Combining Form
Example: osteoarthropathy (ä-stē-ō-är-THROP-ă-thē) – disease of bone and joint
WR CV WR CV S
oste / o / arthr / o /pathy
CF CF
Practice pronouncing and defining these medical terms that are not easily broken into word parts.
adhesion (ad-HĒ-zhŏn)
ascites (ă-SĪT-ēz)
cirrhosis (sĭ-RŌ-sĭs)
Crohn’s disease (krōnz diz-ĒZ′)
dysentery (DIS-ĕn-ter-ē)
emesis (ĔM-ĕ-sĭs)
feces (FĒ-sēz)
flatus (FLĀ-tŭs)
hemorrhoids (HEM-ŏ-royds)
melena (mĕ-LĒ-nă)
nausea (NAW-sē-ă)
obesity (ō-BĒ-sĭt-ē)
palpate (PAL-pāt)
polyp (POL-ĭp)
reflux (RĒ-flŭks)
stoma (STŌ-mă)
Practice pronouncing and defining these commonly abbreviated digestive system terms.
APR (abdominoperineal resection)
BE (barium enema)
EGD (esophagogastroduodenoscopy)
ERCP (endoscopic retrograde cholangiopancreatography)
EUS (endoscopic ultrasound)
FOBT (fecal occult blood test)
GERD (gastroesophageal reflux disease)
GI (gastrointestinal)
H.pylori (Helicobacter pylori)
IBS (irritable bowel syndrome)
N&V (nausea and vomiting)
PEG (percutaneous endoscopic gastrostomy)
UC (ulcerative colitis)
UGI (upper gastrointestinal)
UPPP (uvulopalatopharyngoplasty)
Sort the terms from the word lists above into the following categories.
- Disease and Disorder (terms describing any deviation from normal structure and function)
- Diagnostic (terms related to process of identifying a disease, condition, or injury from its signs and symptoms)
- Therapeutic (terms related to treatment or curing of diseases)
- Anatomic (terms related to body structure)
Use terms related to the digestive system.
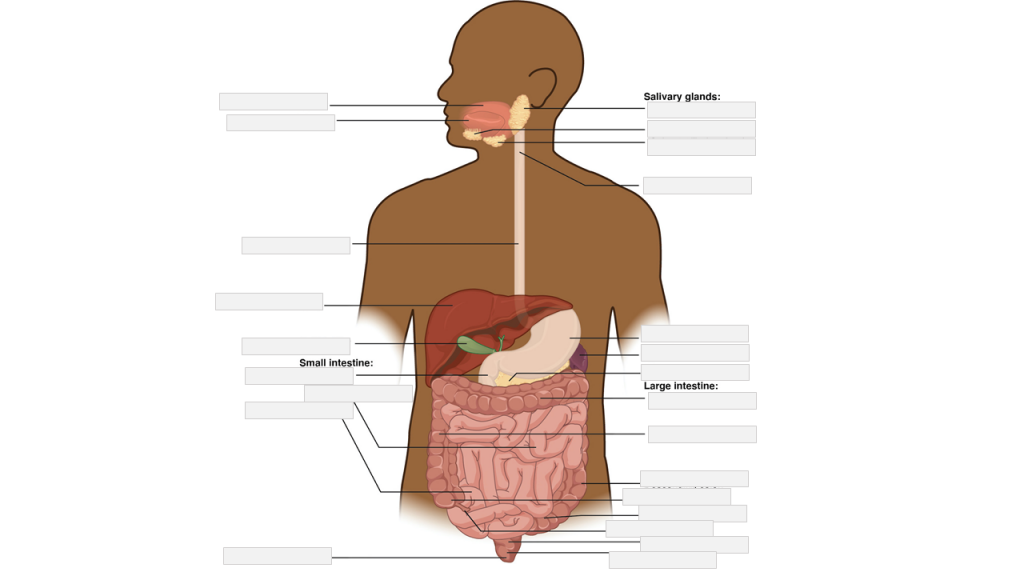
Label the following digestive system anatomy.
anal canal | anus | descending colon | duodenum | esophagus | gallbladder | ileum | jejunum | liver | mouth | parotid gland | pharynx | sigmoid colon | sublingual gland | submandibular gland | tongue | transverse colon
Place the following medical terms in context to complete the scenario below.
adhesion | ascites | cirrhosis | dysentery | emesis | feces | flatus | hemorrhoids | melena | nausea | obesity | palpate | polyp | reflux | stoma
Physician during an examination will ________ to feel for texture, size, consistency and location of body parts with hands.
A ________ is a small tumour like growth that extend from the surface of a mucous membrane. ________ is an abnormal increase in the proportion of fat cells resulting in excess body weight for height.
Distended and swollen veins in the rectum and anus are called ________.
The medical term for vomiting is ________.
________ is black tarry stool that contains blood from the gastrointestinal tract.
________ is the medical term for gas in the gastrointestinal tract.
Abnormal intraperitoneal accumulation of fluid with large amount of proteins and electrolytes is ________.
________ is fecal matter.
Abnormal backward flow is called ________.
The urge to vomit is ________.
________ is a chronic degenerative disease of the liver due to alcohol abuse.
________ is an inflammation of the intestine presenting with abdominal pain and bloody diarrhea.
A band of scar tissue that binds anatomic surfaces to each other is called an ________.
The surgical opening between an organ and the surface of the body is called a ________.
Place the following medical terms in context to complete the scenario below.
diarrhea | electrolytes | eyes | gait | Glucose | resists walking | session | stools | treatment | vomiting
DIGESTIVE SYSTEM – CONSULTATION REPORT
PATIENT NAME: Alex WEBB
AGE: 30
DOB: November 10
SEX: Male
CONSULTANT: Louis D. Wainwright, MD, Gastroenterology
REQUESTING PHYSICIAN: Trevor Sharpe, MD, Family Medicine
REASON FOR CONSULTATION: Please evaluate GI distress.
I was asked to see this 30-year old male in consultation because of unremitting nausea, ________, ________, abdominal pain, dizziness, and low-grade fever. The patient has a poor appetite but reports no weight loss. He has noted some postprandial cramping, midepigastric pain, and unremitting diarrhea but no blood in the ________. He states he is “healthier,” but he still has some dizziness.
Initial treatment consisted of IV fluids and control of ________. Thereafter, the patient was progressed to clear fluids and soft diet. He has done well on this routine; however, his dizziness has persisted. Fever has resolved.
On admission, the patient’s lab data revealed CBC with hematocrit of 142, hemoglobin 25 with differential of neutrophils 51%, bands 8%, lymphocytes 26%, monocytes 6%, basophils none. Serum electrolytes were normal. Potassium was low at 3.5, BUN: creatinine ratio was normal. ________ was within normal range. Stool studies were within normal.
On examination, I find the patient to be lethargic and uncomfortable with mild nausea and dizziness. He prefers to keep his eyes closed. On examination of the ________ , I find no nystagmus. There is pallor to the skin, and he seems cool to the touch. Upon standing by the bedside, the patient is unsteady. Although he ________, when he attempts to walk, his ________ is halting, and he tends to fall to the left side. Abdomen is flat and nontender. Bowel sounds are WNL. Rectal exam deferred.
RECOMMENDATIONS: I think we should continue essential ________ of this gentleman. Because of the symptoms of dizziness on admission, we may want to consider a CT scan to rule out an intracerebral bleed or subdural hematoma. My opinion at this time is that we are dealing with a resolving ________ of gastritis.
Thank you for asking me to see this patient. I will be glad to follow him with you throughout his hospital stay.
____________________________________
Louis D. Wainwright, MD, Gastroenterology
Place the following medical terms in context to complete the scenario below.
antrum | bleeding | duodenum | duodenitis | esophagitis | GE | lateral | Lidocaine | Retroflexion | sporadic | stomach | ulceration
DIGESTIVE SYSTEM – OPERATIVE REPORT
PATIENT NAME: Bruce WEBSTER
AGE: 48
SEX: Male
DOB: September 23
DATE OF ADMISSION: July 2
DATE OF PROCEDURE: July 2
ADMITTING PHYSICIAN: Trevor Sharpe, MD, Family Medicine
SURGEON: Louis D. Wainwright, MD, Gastroenterology
PREOPERATIVE DIAGNOSIS: GI Bleed.
POSTOPERATIVE DIAGNOSES:
1. Severe ________.
2. Gastroesophageal ________.
3. No Significant bleeding seen in the stomach.
OPERATIVE PROCEDURE: Gastrointestinal endoscopy.
ANESTHESIA: ________ 1%.
PROCEDURE: The patient was placed into the left ________ position. A scope was introduced from the mouth, under visualization and advanced to the upper part of the ________, upper part of esophagus, middle of esophagus, ________ junction, and some ________ bleeding was seen at the GE junction. The scope was moved through the upper part of the stomach into the ________. The ________ showed some inflammation and the scope was then brought out. ________ was not performed. The scope was then brought back slowly. Mild ________ was also seen and a little bit of ulceration noted at GE junction.
CONCLUSION: Severe esophagitis, may be some source of ________ from there, but no active bleeding at this time.
________________________________________
Louis D. Wainwright, MD, Gastroenterology
Test your knowledge by answering the questions below.
A band of smooth muscle at the junction between the pylorus of the stomach and the duodenum of the small intestine…
- Quadrate
- Ampulla
- Pyloric sphincter
Fatty tissue that stretches over the abdomen, plays a role in immune response and the growth of certain cancers…
- Convex
- Fundus
- Omentum
The process of breaking down the fat into smaller blood cells which makes it easy for enzymes to function and digest food…
- Emulsification
- Malabsorption
- Bicarbonate
Location where the diaphragm has a small opening through which the esophagus passes before connecting…
- Hilum
- Hiatal
- Lacteals
Situated nearer to the center of the body or the point of attachment…
- Quadrate
- Proximal
- Distal
