3 Integumentary System
WTCS Learning Objectives
- Apply the rules of medical language to build, analyze, spell, pronounce, abbreviate, and define terms as they relate to the integumentary system
- Identify meanings of key word components of the integumentary system
- Categorize diagnostic, therapeutic, procedural or anatomic terms related to the integumentary system
- Use terms related to the integumentary system
- Use terms related to the diseases and disorders of the integumentary system
Integumentary System Word Parts
Click on prefixes, combining forms, and suffixes to reveal a list of word parts to memorize for the Integumentary System.
Introduction to the Integumentary System
The integumentary system refers to the skin and its accessory structures. In the adult human body, the skin makes up about 16 percent of body weight and covers an area of 16-21 ft2.
In fact, the skin and accessory structures are the largest organ system in the human body. The skin protects your inner organs and it is in need of daily care and protection to maintain its health.
Watch this video:
Media 3.1. The science of skin – Emma Bryce [Video]. Copyright 2018 by Ted-Ed.
Practice integumentary system medical terms.
Anatomy (Structures) of the Integumentary System
The skin and its accessory structures make up the integumentary system, which provides the body with overall protection. The skin is made of multiple layers of cells and tissues, which are held to underlying structures by connective tissue. The deeper layer of skin is well vascularized. It also has numerous sensory, and autonomic and sympathetic nerve fibers ensuring communication to and from the brain.
The skin is composed of two main layers:
- The epidermis
- The dermis
- Beneath the dermis lies the hypodermis
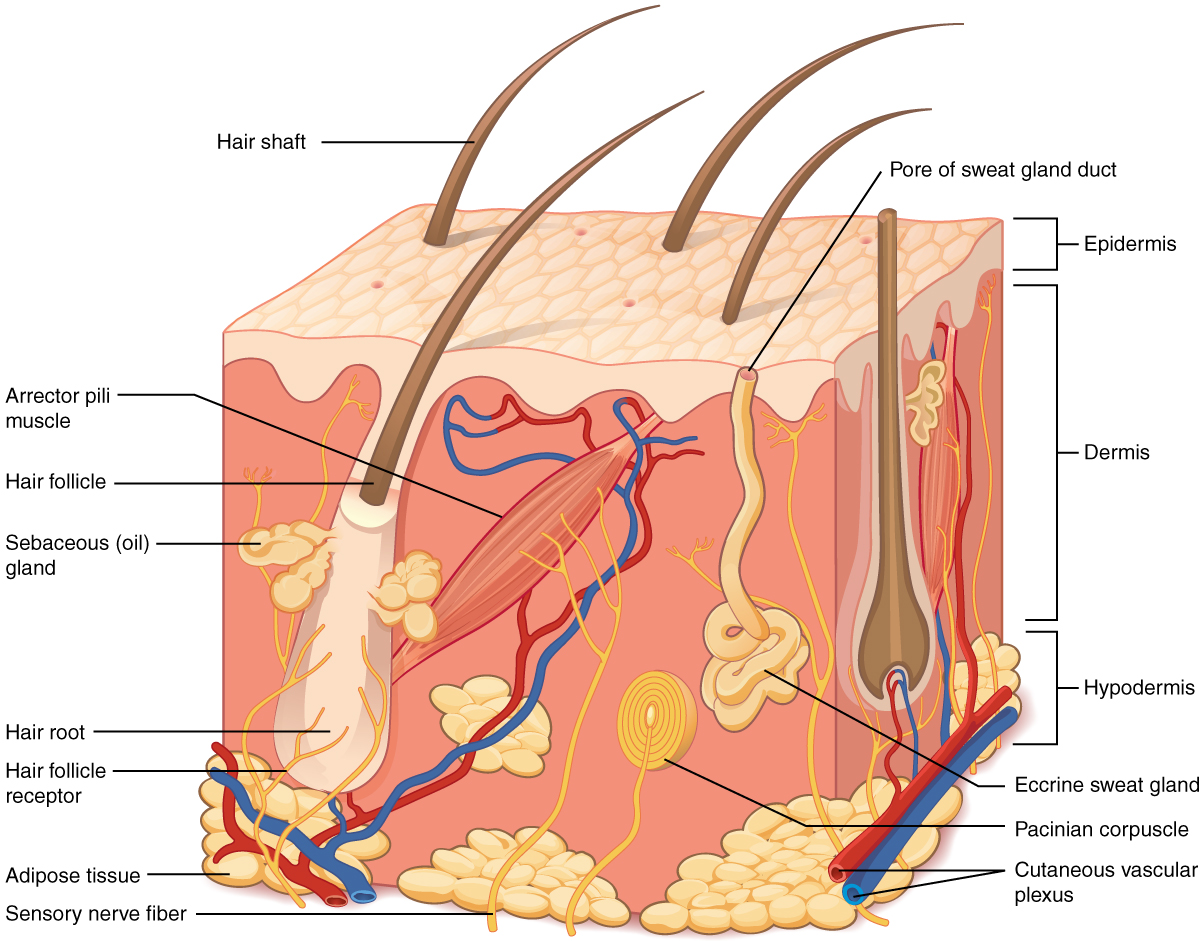
Concept Check
- On the diagram above find the two layers of the skin; epidermis and dermis.
- The literal breakdown for hypodermis is below the dermis. On the diagram above where can you locate it?
- Can you find a hair follicle, hair root and hair shaft?
- Keep reading to find out what the arrector pilli muscle does when you are frightened.
Epidermis
The epidermis is composed of keratinized, stratified squamous epithelium. It is made of four or five layers of epithelial cells, depending on its location in the body. It is avascular.
The cells in all of the layers except the stratum basale are called keratinocytes. Keratin is an intracellular fibrous protein that gives hair, nails, and skin their hardness and water-resistant properties. The keratinocytes in the stratum corneum are dead and regularly slough away, being replaced by cells from the deeper layers.
Dermis
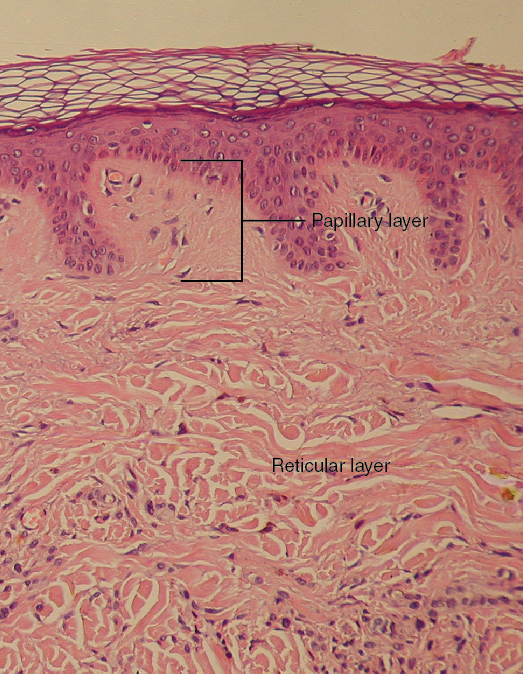
Papillary Layer
The papillary layer is made of loose, areolar connective tissue, which means the collagen and elastin fibers of this layer form a loose mesh. This superficial layer of the dermis projects into the stratum basale of the epidermis to form finger-like dermal papillae (see Figure 3.2). Within the papillary layer are fibroblasts, a small number adipocytes, and an abundance of small blood vessels. In addition, the papillary layer contains phagocytes, that help fight bacteria or other infections that have breached the skin. This layer also contains lymphatic capillaries, nerve fibers, and Meissner corpuscles.
Reticular Layer
Underlying the papillary layer is the much thicker reticular layer, composed of dense, irregular connective tissue. This layer is well vascularized and has a rich sensory and sympathetic nerve supply. The reticular layer appears reticulated due to a tight meshwork of fibers. Elastin fibers provide some elasticity to the skin, enabling movement. Collagen fibers provide structure and tensile strength, with strands of collagen extending into both the papillary layer and the hypodermis. In addition, collagen binds water to keep the skin hydrated. Collagen injections and Retin-A creams help restore skin turgor by either introducing collagen externally or stimulating blood flow and repair of the dermis, respectively.
Hypodermis
The hypodermis serves to connect the skin to the underlying fascia of the bones and muscles. It is not strictly a part of the skin, although the border between the hypodermis and dermis can be difficult to distinguish. The hypodermis consists of well-vascularized, loose, areolar connective tissue and [pb_glossary id="1697"]adipose[/pb_glossary] tissue, which functions as a mode of fat storage and provides insulation and cushioning for the integument.
Practice labeling the layers of the skin.
Physiology (Function) of the Integumentary System
The skin and accessory structures perform a variety of essential functions, such as protecting the body from invasion by microorganisms, chemicals, and other environmental factors; preventing dehydration; acting as a sensory organ; modulating body temperature and electrolyte balance; and synthesizing vitamin D. The underlying hypodermis has important roles in storing fats, forming a “cushion” over underlying structures, and providing insulation from cold temperatures.
Protection
The skin protects the body from wind, water, and UV sunlight. It acts as a protective barrier against water loss and it also is the first line of defense against abrasive activity such as grit, microbes, or harmful chemicals. Sweat excreted from sweat glands deters microbes from over-colonizing the skin surface.
Sensory Function
The skin acts as a sense organ because the epidermis, dermis, and the hypodermis contain specialized sensory nerve structures that detect touch, surface temperature, and pain. These receptors are more concentrated on the tips of the fingers, which are most sensitive to touch, especially the Meissner corpuscle, which responds to light touch, and the Pacinian corpuscle , which responds to vibration. Merkel cells, seen scattered in the stratum basale, are also touch receptors. In addition to these specialized receptors, there are sensory nerves connected to each hair follicle, pain and temperature receptors scattered throughout the skin, and motor nerves innervate the arrector pili muscles and glands. This rich innervation helps us sense our environment and react accordingly,
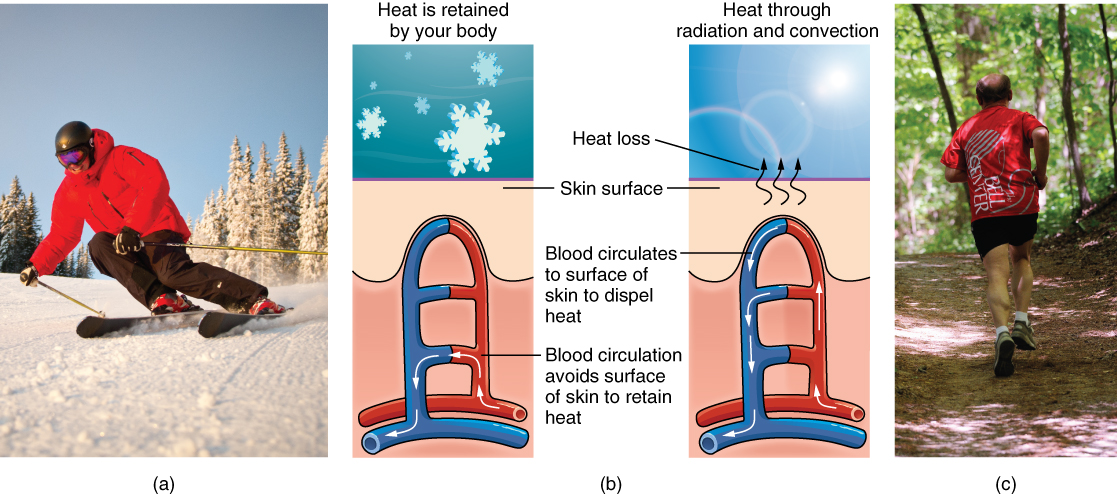
Thermoregulation
The integumentary system helps regulate body temperature through its tight association with the sympathetic nervous system. The sympathetic nervous system is continuously monitoring body temperature and initiating appropriate motor responses.
- When the body becomes warm sweat glands, accessory structures to the skin, secrete water, salt, and other substances to cool the body.
- Even when the body does not appear to be noticeably sweating, approximately 500 mL of sweat are secreted a day.
- If the body becomes excessively warm due to high temperatures, vigorous activity, or a combination of the two, sweat glands will be stimulated by the sympathetic nervous system to produce large amounts of sweat.
- When the sweat evaporates from the skin surface, the body is cooled as body heat is dissipated.
- In addition to sweating, arterioles in the dermis dilate so that excess heat carried by the blood can dissipate through the skin and into the surrounding environment.
- This accounts for the skin redness that many people experience when exercising.
- When body temperatures drop, the arterioles constrict to minimize heat loss, particularly in the ends of the digits and tip of the nose.
- This reduced circulation can result in the skin taking on a whitish hue.
- Although the temperature of the skin drops as a result, passive heat loss is prevented, and internal organs and structures remain warm.
- If the temperature of the skin drops too much (such as environmental temperatures below freezing), the conservation of body core heat can result frostbite .
Concept Check
Can you describe the thermoregulation process between the integumentary system and the sympathetic system?
- When body temperature is too warm.
- When body temperature is too cold.
Vitamin D Synthesis
The epidermal layer of human skin synthesizes Vitamin D when exposed to UV radiation. In the presence of sunlight, a form of Vitamin D3 called cholecalciferol is synthesized from a derivative of the steroid cholesterol in the skin. The liver converts cholecalciferol to calcidiol, which is then converted to calcitriol (the active chemical form of the vitamin) in the kidneys.
- Vitamin D is essential for normal absorption of calcium and phosphorous, which are required for healthy bones.
- The absence of sun exposure can lead to a lack of vitamin D in the body, in children this can cause rickets. Vitamin D deficiency in elderly individuals may lead to osteomalacia.
- In present day society, Vitamin D is added as a supplement to many foods, including milk and orange juice, compensating for the need for sun exposure. In addition to its essential role in bone health, Vitamin D is essential for general immunity against bacterial, viral, and fungal infections.
Watch this video:
Media 3.2. The Integumentary System, Part 2 – Skin Deeper: Crash Course A&P #7 [Online video]. Copyright 2015 by CrashCourse.Media 3.2. The Integumentary System, Part 2 – Skin Deeper: Crash Course A&P #7 [Online video]. Copyright 2015 by CrashCourse.
Accessory Structures
Accessory structures of the skin include hair, nails, sweat glands, and sebaceous glands. These structures embryologically originate from the epidermis and can extend down through the dermis into the hypodermis.
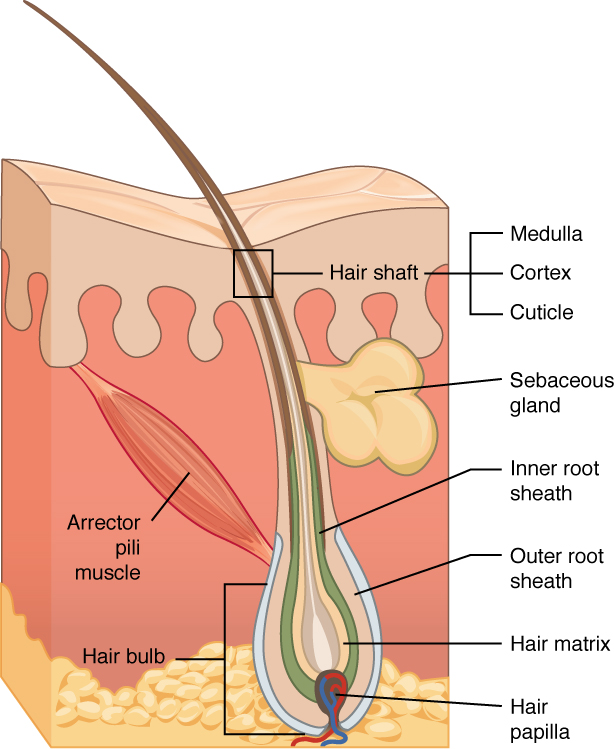
Hair
Hair is a keratinous filament growing out of the epidermis. It is primarily made of dead, keratinized cells. Strands of hair originate in an epidermal penetration of the dermis called the hair follicle. The hair shaft is the part of the hair not anchored to the follicle, and much of this is exposed at the skin’s surface. The rest of the hair, which is anchored in the follicle, lies below the surface of the skin and is referred to as the hair root. The hair root ends deep in the dermis at the hair bulb, and includes a layer of mitotically active basal cells called the hair matrix. The hair bulb surrounds the hair papilla, which is made of connective tissue and contains blood capillaries and nerve endings from the dermis (see Figure 3.4).
Hair Function
Hair serves a variety of functions, including protection, sensory input, thermoregulation, and communication. For example:
- Hair on the head protects the skull from the sun.
- Hair in the nose and ears, and around the eyes (eyelashes) defends the body by trapping and excluding dust particles that may contain allergens and microbes.
- Hair of the eyebrows prevents sweat and other particles from dripping into and bothering the eyes.
Hair also has a sensory function due to sensory innervation by a hair root plexus surrounding the base of each hair follicle. Hair is extremely sensitive to air movement or other disturbances in the environment, much more so than the skin surface. This feature is also useful for the detection of the presence of insects or other potentially damaging substances on the skin surface.
Each hair root is connected to a smooth muscle called the arrector pili that contracts in response to nerve signals from the sympathetic nervous system, making the external hair shaft “stand up.” The primary purpose for this is to trap a layer of air to add insulation. This is visible in humans as goose bumps and even more obvious in animals, such as when a frightened cat raises its fur. Of course, this is much more obvious in organisms with a heavier coat than most humans, such as dogs and cats.
Hair Growth, Loss and Color
Hair grows and is eventually shed and replaced by new hair. Hair typically grows at the rate of 0.3 mm per day. On average, 50 hairs are lost and replaced per day. Hair loss occurs if there is more hair shed than what is replaced and can happen due to hormonal or dietary changes. Hair loss can also result from the aging process, or the influence of hormones. Similar to the skin, hair gets its color from the pigment melanin, produced by melanocytes in the hair papilla. Different hair color results from differences in the type of melanin. As a person ages, the melanin production decreases, and hair tends to lose its color and becomes gray and/or white.
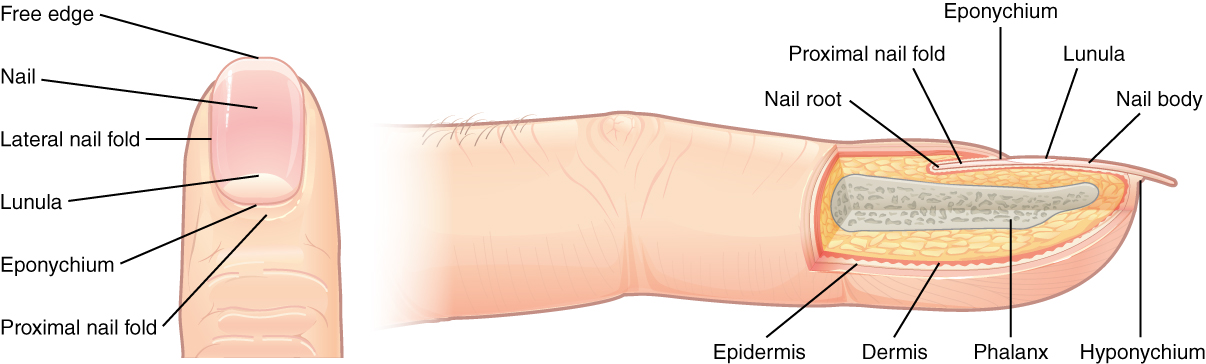
Nails
The nail bed is a specialized structure of the epidermis that is found at the tips of our fingers and toes. The nail body is formed on the nail bed, and protects the tips of our fingers and toes as they are the farthest extremities and the parts of the body that experience the maximum mechanical stress (see Figure 3.5). The nail body forms a back-support for picking up small objects with the fingers. The nail body is composed of densely packed dead keratinocytes.
The epidermis in this part of the body has evolved a specialized structure upon which nails can form. The nail body forms at the nail root, which has a matrix of proliferating cells from the stratum basale that enables the nail to grow continuously. The lateral nail fold overlaps the nail on the sides, helping to anchor the nail body. The nail fold that meets the proximal end of the nail body forms the nail cuticle, also called the eponychium.
The nail bed is rich in blood vessels, making it appear pink, except at the base, where a thick layer of epithelium over the nail matrix forms a crescent-shaped region called the lunula (the “little moon”). The area beneath the free edge of the nail, furthest from the cuticle, is called the hyponychium. It consists of a thickened layer of stratum corneum.
Sweat Glands
Sudoriferous Glands
When the body becomes warm, sudoriferous glands produce sweat to cool the body. Sweat glands develop from epidermal projections into the dermis and are classified as merocrine glands; that is, the secretions are excreted by exocytosis through a duct without affecting the cells of the gland. There are two types of sweat glands, each secreting slightly different products.
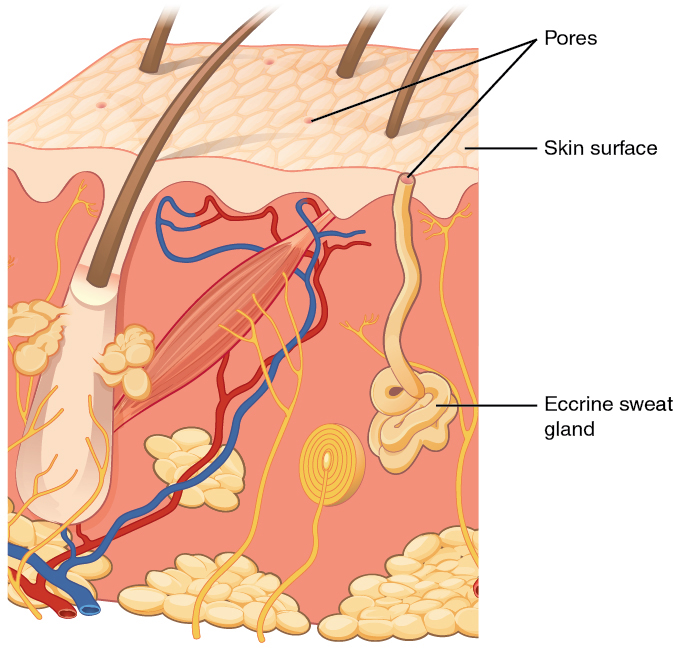
An eccrine sweat gland is type of gland that produces a hypotonic sweat for thermoregulation as described previously. These glands are found all over the skin’s surface, but are especially abundant on the palms of the hand, the soles of the feet, and the forehead (Figure 3.6). They are coiled glands lying deep in the dermis, with the duct rising up to a pore on the skin surface, where the sweat is released. This type of sweat, released by exocytosis, is hypotonic and composed mostly of water, with some salt, antibodies, traces of metabolic waste, and dermicidin, an antimicrobial peptide. Eccrine glands are a primary component of thermoregulation in humans and thus help to maintain homeostasis .
An apocrine sweat gland is usually associated with hair follicles in densely hairy areas, such as armpits and genital regions. Apocrine sweat glands are larger than eccrine sweat glands and lie deeper in the dermis, sometimes even reaching the hypodermis, with the duct normally emptying into the hair follicle. In addition to water and salts, apocrine sweat includes organic compounds that make the sweat thicker and subject to bacterial decomposition and subsequent smell. The release of this sweat is under both nervous and hormonal control, and plays a role in the poorly understood human pheromone response. Most commercial antiperspirants use an aluminum-based compound as their primary active ingredient to stop sweat. When the antiperspirant enters the sweat gland duct, the aluminum-based compounds precipitate due to a change in pH and form a physical block in the duct, which prevents sweat from coming out of the pore.
Sebaceous Glands
A sebaceous gland is a type of oil gland that is found all over the body and helps to lubricate and waterproof the skin and hair. Most sebaceous glands are associated with hair follicles. They generate and excrete sebum, a mixture of lipids, onto the skin surface, thereby naturally lubricating the dry and dead layer of keratinized cells of the stratum corneum, keeping it pliable. The fatty acids of sebum also have antibacterial properties, and prevent water loss from the skin in low-humidity environments. The secretion of sebum is stimulated by hormones, many of which do not become active until puberty. Thus, sebaceous glands are relatively inactive during childhood.
Words not Easily Broken into Word Parts
Common Integumentary System Abbreviations
Many terms and phrases related to the integumentary system are abbreviated. Learn these common abbreviations by expanding the list below.
Changes Due to Aging
All systems in the body accumulate subtle and some not-so-subtle changes as a person ages. Among these changes are reductions in cell division, metabolic activity, blood circulation, hormonal levels, and muscle strength (see Figure 3.7). In the skin, these changes are reflected in decreased mitosis in the stratum basale, leading to a thinner epidermis. The dermis, which is responsible for the elasticity and resilience of the skin, exhibits a reduced ability to regenerate, which leads to slower wound healing. The hypodermis, with its fat stores, loses structure due to the reduction and redistribution of fat, which in turn contributes to the thinning and sagging of skin.

The accessory structures also have lowered activity, generating thinner hair and nails, and reduced amounts of sebum and sweat. A reduced sweating ability can cause some elderly to be intolerant to extreme heat. Other cells in the skin, such as melanocytes and dendritic cells, also become less active, leading to a paler skin tone and lowered immunity. Wrinkling of the skin occurs due to breakdown of its structure, which results from decreased collagen and elastin production in the dermis, weakening of muscles lying under the skin, and the inability of the skin to retain adequate moisture.
Disease and Disorders
The integumentary system is susceptible to a variety of diseases, disorders, and injuries. These range from annoying but relatively benign bacterial or fungal infections that are categorized as disorders, to skin cancer and severe burns, which can be fatal. In this section, you will learn several of the most common skin conditions.
One of the most talked about diseases is skin cancer. Most cancers are identified by the organ or tissue in which the cancer originates. One common form of cancer is skin cancer.
In general, cancers result from an accumulation of DNA mutations. These mutations can result in cell populations that do not die when they should and uncontrolled cell proliferation that leads to tumors. Although many tumors are benign, some metastasize. Cancers are characterized by their ability to metastasize.
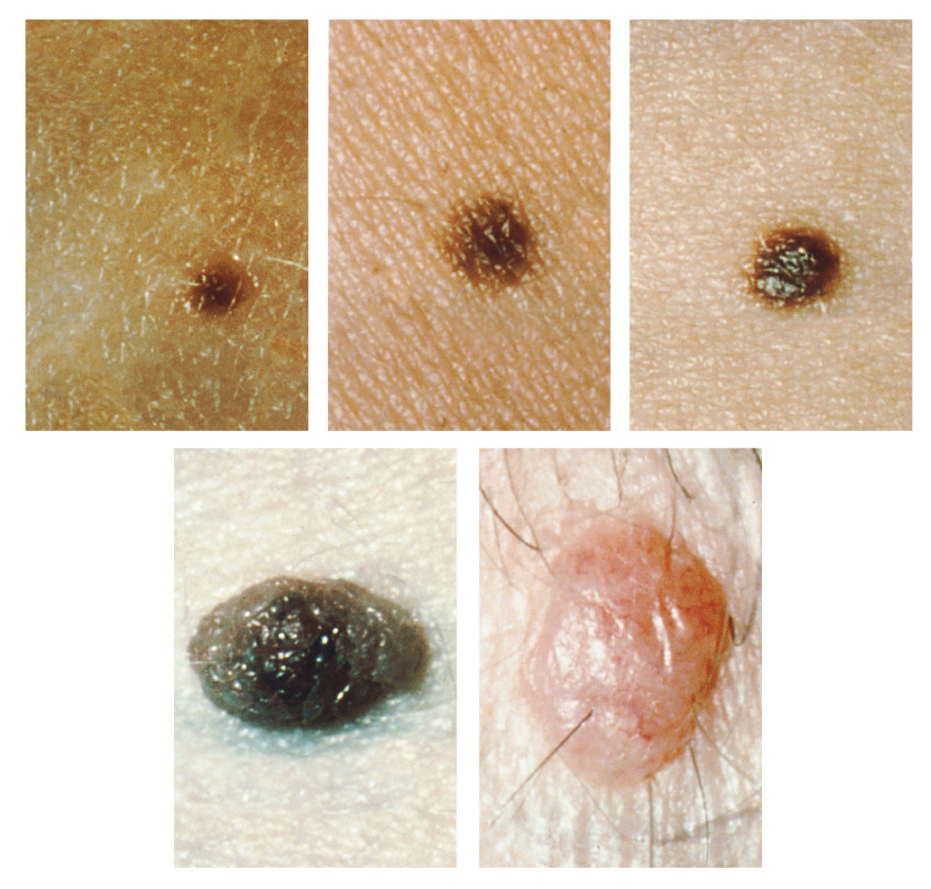
Sun Damage
It requires about 10 days after initial sun exposure for melanin synthesis to peak, which is why pale-skinned individuals tend to suffer sunburns of the epidermis initially. Dark-skinned individuals can also get sunburns, but are more protected than are pale-skinned individuals. Too much sun exposure can eventually lead to wrinkling due to the destruction of the cellular structure of the skin, and in severe cases, can cause sufficient DNA damage to result in skin cancer. When there is an irregular accumulation of melanocytes in the skin, freckles appear. Moles are larger masses of melanocytes, and although most are benign, they should be monitored for changes that might indicate the presence of cancer (see Figure 3.8).
Basal Cell Carcinoma (BCC)
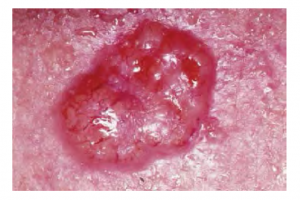
Basal cell carcinoma is a form of cancer that affects the mitotically active stem cells in the stratum basale of the epidermis. It is the most common of all cancers that occur in the United States and is frequently found on the head, neck, arms, and back, which are are as that are most susceptible to long-term sun exposure. Although UV rays are the main culprit, exposure to other agents, such as radiation and arsenic, can also lead to this type of cancer. Wounds on the skin due to open sores, tattoos, burns, etc. may be predisposing factors. Basal cell carcinomas start in the stratum basale and usually spread along this boundary. At some point, they begin to grow toward the surface and become an uneven patch, bump, growth, or scar on the skin surface (see Figure 3.9). Like most cancers, basal cell carcinomas respond best to treatment when caught early. Treatment options include surgery, freezing (cryosurgery), and topical ointments.
Squamous Cell Carcinoma (SCC)

Squamous cell carcinoma is a cancer that affects the keratinocytes of the stratum spinosum and presents as lesions commonly found on the scalp, ears, and hands (see Figure 3.10). It is the second most common skin cancer. The American Cancer Society reports that two of 10 skin cancers are squamous cell carcinomas, and it is more aggressive than basal cell carcinoma. If not removed, these carcinomas can metastasize. Surgery and radiation are used to cure squamous cell carcinoma.
Melanoma
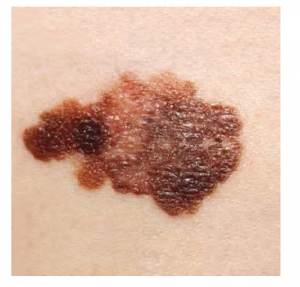
A melanoma is a cancer characterized by the uncontrolled growth of melanocytes, the pigment-producing cells in the epidermis. Typically, a melanoma develops from a mole. It is the most fatal of all skin cancers, as it is highly metastatic and can be difficult to detect before it has spread to other organs. Melanomas usually appear as asymmetrical brown and black patches with uneven borders and a raised surface (see Figure 3.11). Treatment typically involves surgical excision and immunotherapy.
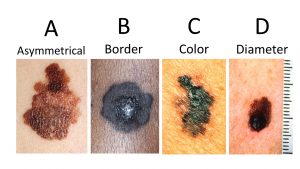
ABCDE for Early Diagnosis
Doctors often give their patients the following ABCDE mnemonic to help with the diagnosis of early-stage melanoma (see Fig 3.12). If you observe a mole on your body displaying these signs, consult a doctor.
- Asymmetry – the two sides are not symmetrical
- Borders – the edges are irregular in shape
- Color – the color is varied shades of brown or black
- Diameter – it is larger than a pencil eraser
- Evolving – its shape has changed
Some specialists cite the following additional signs for the most serious form, nodular melanoma:
Elevated – it is raised on the skin surface
Firm – it feels hard to the touch
Growing – it is getting larger
Albinism
Albinism is a genetic disorder that affects (completely or partially) the coloring of skin, hair, and eyes. This is primarily due to the inability of melanocytes to produce melanin. Individuals with albinism tend to appear white or very pale due to the lack of melanin in their skin and hair. Recall that melanin helps protect the skin from the harmful effects of UV radiation. Individuals with albinism tend to need more protection from UV radiation, as they are more prone to sunburns and skin cancer. They also tend to be more sensitive to light and have vision problems due to the lack of pigmentation on the retinal wall (Betts, et al., 2021)
Treatment of this disorder usually involves addressing the symptoms, such as limiting UV light exposure to the skin and eyes. In vitiligo, the melanocytes in certain areas lose their ability to produce melanin, possibly due to an autoimmune reaction. This leads to a loss of color in patches (see Figure 3.13). Neither albinism nor vitiligo directly affects the lifespan of an individual (Betts, et al., 2021)

Changes in Skin Coloration
Other changes in the appearance of skin coloration can be indicative of diseases associated with other body systems.
- Liver disease or liver cancer can cause the accumulation of bile and the yellow pigment bilirubin, leading to xanthoderma or jaundice.
- Tumors of the pituitary gland can result in the secretion of large amounts of melanocyte-stimulating hormone (MSH), which results in a darkening of the skin.
- Addison’s disease can stimulate the release of excess amounts of adrenocorticotropic hormone (ACTH), which can give the skin a deep bronze color
- A sudden drop in oxygenation can affect skin color, causing the skin to initially turn ashen (white).
- A prolonged reduction in oxygen levels, dark red deoxyhemoglobin becomes dominant in the blood, making the skin appear blue, a condition referred to as cyanosis. This happens when the oxygen supply is restricted, as when someone is experiencing difficulty in breathing because of asthma or a heart attack. However, in these cases the effect on skin color has nothing do with the skin’s pigmentation (Betts, et al., 2021)
Skin Disorders
Two common skin disorders are eczema and acne. Eczema is an inflammatory condition and occurs in individuals of all ages. Acne involves the clogging of pores, which can lead to infection and inflammation, and is often seen in adolescents. Other disorders, include seborrheic dermatitis (on the scalp), psoriasis, fungal infections, cold sores, impetigo, scabies, hives, and warts (Betts, et al., 2021).
Eczema

Eczema is an allergic reaction that manifests as dry, itchy patches of skin that resemble rashes (see Figure 3.14). It may be accompanied by swelling of the skin, flaking, and in severe cases, bleeding. Symptoms are usually managed with moisturizers, corticosteroid creams, and immunosuppressants (Betts, et al., 2021).
Acne
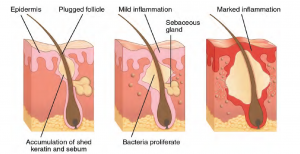
Acne is a skin disturbance that typically occurs on areas of the skin that are rich in sebaceous glands (face and back). It is most common along with the onset of puberty due to associated hormonal changes, but can also occur in infants and continue into adulthood. Hormones, such as androgens, stimulate the release of sebum. An overproduction and accumulation of sebum along with keratin can block hair follicles. This plug is initially white. The sebum, when oxidized by exposure to air, turns black. Acne results from infection by acne-causing bacteria (Propionibacterium and Staphylococcus), which can lead to redness and potential scarring due to the natural wound healing process (see Figure 3.15) (Betts, et al., 2021).
Ringworm
Tinea or dermatophytosis is often referred to as ringworm. Ringworm presents as a circular rash that is itchy and red and can be found on various parts of the body. It is referred to by the location that it is found:
-
- Tinea Pedis – feet or commonly referred to as athlete’s feet
- Tinea Capitis – scalp
- Tinea barbae – beard
- Tinea manuum – hands
- Tinea unguium – Toenails and fingernails also called onychomycosis
- Tinea corporis – Body parts such as arms and legs (Center for Disease Control and Prevention, 2018a)
To learn more about ringworm, visit the Center for Disease Control and Prevention’s web page on fungal infections.
Psoriasis
Psoriasis is a chronic autoimmune disorder that results in patches of thick red skin with the appearance of silvery scales. These patches can be found on elbows, knees, scalp, low back, face, feet, fingernails, toenails and even the mouth. Psoriasis can be confused with other skin disease so a dermatologist is the best physician to diagnosis psoriasis. Treatments may include creams, ointments, ultraviolet light therapy and medication (Center for Disease Control and Prevention, 2018). To learn more, visit the Center for Disease Control and Prevention’s web page on psoriasis.
Injuries
Skin injuries set off a healing process that occurs in several overlapping stages.
- The first step to repairing damaged skin is the formation of a blood clot that helps stop the flow of blood and scabs over with time. Many different types of cells are involved in wound repair, especially if the surface area that needs repair is extensive.
- Before the basal stem cells of the stratum basale can recreate the epidermis, fibroblasts mobilize and divide rapidly to repair the damaged tissue by collagen deposition, forming granulation tissue.
- Blood capillaries follow the fibroblasts and help increase blood circulation and oxygen supply to the area.
- Immune cells, such as macrophages, roam the area and engulf any foreign matter to reduce the chance of infection (Betts, et al., 2021).
Burns
A burn results when the skin is damaged by intense heat, radiation, electricity, or chemicals. The damage results in the death of skin cells, which can lead to a massive loss of fluid. Dehydration, electrolyte imbalance, and renal and circulatory failure follow, which can be fatal. Burn patients are treated with intravenous fluids to offset dehydration, as well as intravenous nutrients that enable the body to repair tissues and replace lost proteins. Another serious threat to the lives of burn patients is infection. Burned skin is extremely susceptible to bacteria and other pathogens, due to the loss of protection by intact layers of skin (Betts, et al., 2021).
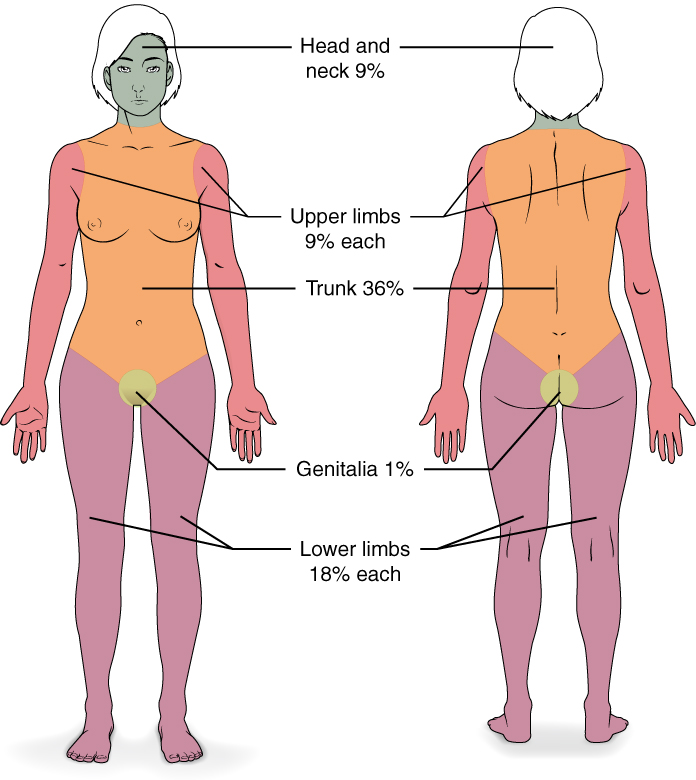
Burn Classification
Burns are sometimes measured in terms of the size of the total surface area affected. This is referred to as the rule of nines, which associates specific anatomical areas with a percentage that is a factor of nine (see Figure 3.16) (Betts, et al., 2021).
Burns are also classified by the degree of their severity.
- A first-degree burn is a superficial burn that affects only the epidermis. Although the skin may be painful and swollen, these burns typically heal on their own within a few days. Mild sunburn fits into the category of a first-degree burn.
- A second-degree burn goes deeper and affects both the epidermis and a portion of the dermis. These burns result in swelling and a painful blistering of the skin. It is important to keep the burn site clean and sterile to prevent infection. If this is done, the burn will heal within several weeks.
- A third-degree burn fully extends into the epidermis and dermis, destroying the tissue and affecting the nerve endings and sensory function. These are serious burns that may appear white, red, or black; they require medical attention and will heal slowly without it.
- A fourth-degree burn is even more severe, affecting the underlying muscle and bone.
Oddly, third and fourth-degree burns are usually not as painful because the nerve endings themselves are damaged. Full-thickness burns cannot be repaired by the body, because the local tissues used for repair are damaged and require debridement, or amputation in severe cases, followed by grafting of the skin from an unaffected part of the body, or from skin grown in tissue culture for grafting purposes. Skin grafts are required when the damage from trauma or infection cannot be closed with sutures or staples (Betts et al., 2021).
Scars and Keloids
Most cuts or wounds, with the exception of ones that only scratch the epidermis, lead to scar formation. Scarring occurs in cases in which there is repair of skin damage, but the skin fails to regenerate the original skin structure. Fibroblasts generate scar tissue in the form of collagen, and the bulk of repair is due to the basket-weave pattern generated by collagen fibers and does not result in regeneration of the typical cellular structure of skin. Instead, the tissue is fibrous in nature and does not allow for the regeneration of accessory structures, such as hair follicles, sweat glands, or sebaceous glands (Betts, et al., 2021).
Sometimes, there is an overproduction of scar tissue, because the process of collagen formation does not stop when the wound is healed; this results in a keloid (see Figure 3.17). In contrast, scars that result from acne and chickenpox have a sunken appearance and are called atrophic scars (Betts, et al., 2021).

Scarring of skin after wound healing is a natural process and does not need to be treated further. Application of mineral oil and lotions may reduce the formation of scar tissue. However, modern cosmetic procedures, such as dermabrasion, laser treatments, and filler injections have been invented as remedies for severe scarring. All of these procedures try to reorganize the structure of the epidermis and underlying collagen tissue to make it look more natural (Betts, et al., 2021).
Bedsores and Stretch Marks
Skin and its underlying tissue can be affected by excessive pressure. One example of this is called a bedsore. Bedsores, also called decubitis ulcers, are caused by constant, long-term, unrelieved pressure on certain body parts that are bony, reducing blood flow to the area and leading to necrosis . Bedsores are most common in elderly patients who have debilitating conditions that cause them to be immobile. Most hospitals and long-term care facilities have the practice of turning the patients every few hours to prevent the incidence of bedsores. If left untreated bedsores can be fatal if they become infected (Betts, et al., 2021)
The skin can also be affected by pressure associated with rapid growth. A stretch mark results when the dermis is stretched beyond its limits of elasticity, as the skin stretches to accommodate the excess pressure. Stretch marks usually accompany rapid weight gain during puberty and pregnancy. They initially have a reddish hue, but lighten over time. Other than for cosmetic reasons, treatment of stretch marks is not required. They occur most commonly over the hips and abdomen (Betts, et al., 2021). For detailed images of types of bedsores, see Minnesota Hospital Association’s Pressure Ulcer Staging Cards.
Calluses
When you wear shoes that do not fit well and are a constant source of abrasion on your toes, you tend to form a callus at the point of contact. This occurs because the basal stem cells in the stratum basale are triggered to divide more often to increase the thickness of the skin at the point of abrasion to protect the rest of the body from further damage. This is an example of a minor or local injury, and the skin manages to react and treat the problem independent of the rest of the body. Calluses can also form on your fingers if they are subject to constant mechanical stress, such as long periods of writing, playing string instruments, or video games. A corn is a specialized form of callus. Corns form from abrasions on the skin that result from an elliptical-type motion (Betts, et al., 2021).
Medical Terms in Context
Medical Specialties and Procedures Related to the Integumentary System
A dermatologist is a medical doctor with specialized training in treating diseases, disorders and injuries related to the integumentary system and its accessory structures. There are many dermatologic subspecialties such as cosmetic dermatology, dermatopathology and pediatric dermatology. To learn more visit the ‘What is a Dermatologist?’ page of the American Academy of Dermatology Association website.
Dermatologists can be specially trained to perform a procedure called Mohs surgery. Mohs surgery excises skin cancers in thin layers until all cancer is removed from the tissue (Mayo Clinic Staff, 2017). For more details about each step of the process visit the Skin Cancer Foundation’s site on Mohs Surgery.
Test Yourself
References
Centers for Disease Control and Prevention. (2018, October 25). Psoriasis. Centers for Disease Control and Prevention: Fungal Diseases. https://www.cdc.gov/psoriasis/
Centers for Disease Control and Prevention. (2018a, August 6). Ringworm. Centers for Disease Control and Prevention: Fungal Diseases. https://www.cdc.gov/fungal/diseases/ringworm/definition.html
CrashCourse. (2015, February 16). The Integumentary system, part 2 – skin deeper: Crash Course A&P #7 [Video]. YouTube. https://youtu.be/EN-x-zXXVwQ
Mayo Clinic Staff. (2017, September 6). Mohs surgery. Mayo Clinic. https://www.mayoclinic.org/tests-procedures/mohs-surgery/about/pac-20385222#:~:text=Mohs%20surgery%20is%20a%20precise,known%20as%20Mohs%20micrographic%20surgery.
Ted-Ed. (2018). The science of skin- Emma Bryce [Video]. https://www.youtube.com/watch?v=OxPlCkTKhzY&t=1s
Unless otherwise indicated, this chapter contains material adapted from Anatomy and Physiology (on OpenStax), by Betts, et al. and is used under a a CC BY 4.0 international license. Download and access this book for free at https://openstax.org/books/anatomy-and-physiology/pages/1-introduction.
has numerous blood vessels
unconsciously regulates
flight or fight response
outer layer of skin, made of closely packed epithelial cells
The layer that is made of dense, irregular connective tissue that houses blood vessels, hair follicles, sweat glands, and other structures
Literally means below the dermis. The layer of the skin below the dermis that is composed mainly of loose connective and fatty tissues
without blood vessels
WTCS Learning Objectives
- Apply the rules of medical language to build, analyze, spell, pronounce, abbreviate, and define terms as they relate to the urinary system
- Identify meanings of key word components of the urinary system
- Categorize diagnostic, therapeutic, procedural or anatomic terms related to the urinary system
- Use terms related to the urinary system
- Use terms related to the diseases and disorders of the urinary system
Urinary System Word Parts
Click on prefixes, combining forms, and suffixes to reveal a list of word parts to memorize for the urinary system.
Introduction to the Urinary System
The urinary system has roles you may be well aware of. Cleansing the blood and ridding the body of wastes probably come to mind. However, there are additional, equally important functions, played by the system. Take, for example, regulation of pH, a function shared with the lungs and the buffers in the blood. Additionally, the regulation of blood pressure is a role shared with the heart and blood vessels. What about regulating the concentration of solutes in the blood? Did you know that the kidney is important in determining the concentration of red blood cells? Eighty-five percent of the erythropoietin (EPO) produced to stimulate red blood cell production is produced in the kidneys. The kidneys also help control blood pressure by producing the enzyme renin . Additionally, the kidneys perform the final synthesis step of vitamin D production, converting calcidiol to calcitriol, the active form of vitamin D. If the kidneys fail, these functions are compromised or lost altogether, with devastating effects on homeostasis.
Watch this video:
Media 8.1. Urinary System, Part 1: Crash Course A&P #38 [Online video]. Copyright 2015 by CrashCourse.
Urinary System Medical Terms
Anatomy (Structures) of the Urinary System
Kidney(s)
The kidneys lie on either side of the spine in the retroperitoneal space between the parietal peritoneum and the posterior abdominal wall, well protected by muscle, fat, and ribs. They are roughly the size of your fist. The male kidney is typically a bit larger than the female kidney. The kidneys are well vascularized, receiving about twenty-five percent of the cardiac output at rest. Figure 8.1 displays the location of the kidneys.
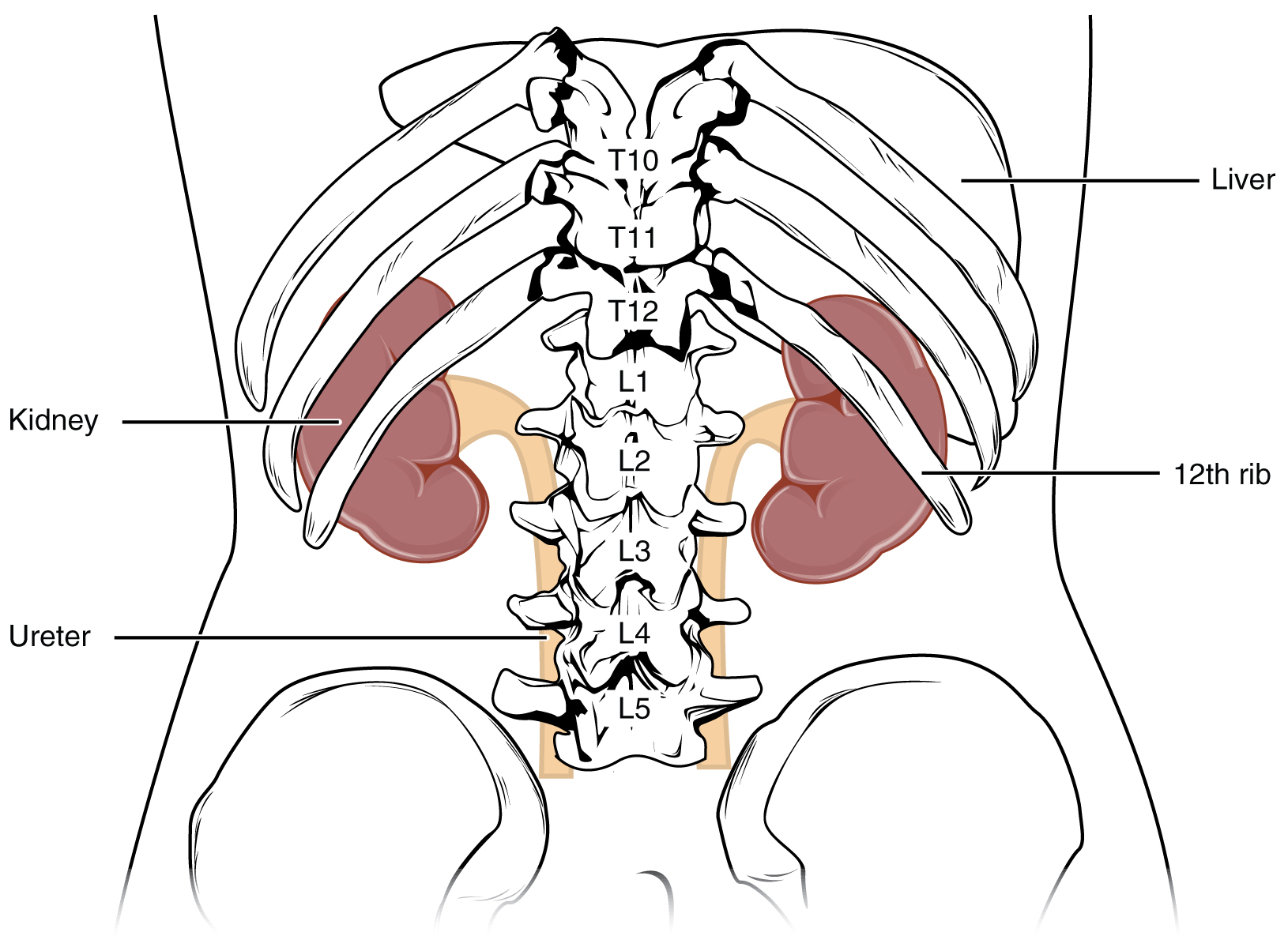
Kidneys' Internal Structure
A frontal section through the kidney reveals an outer region called the renal cortex and an inner region called the medulla (see Figure 8.2). The renal columns are connective tissue extensions that radiate downward from the cortex through the medulla to separate the most characteristic features of the medulla, the renal pyramids and renal papillae. The papillae are bundles of collecting ducts that transport urine made by nephrons to the calyces of the kidney for excretion. The renal columns also serve to divide the kidney into 6–8 lobes and provide a supportive framework for vessels that enter and exit the cortex. The pyramids and renal columns taken together constitute the kidney lobes.
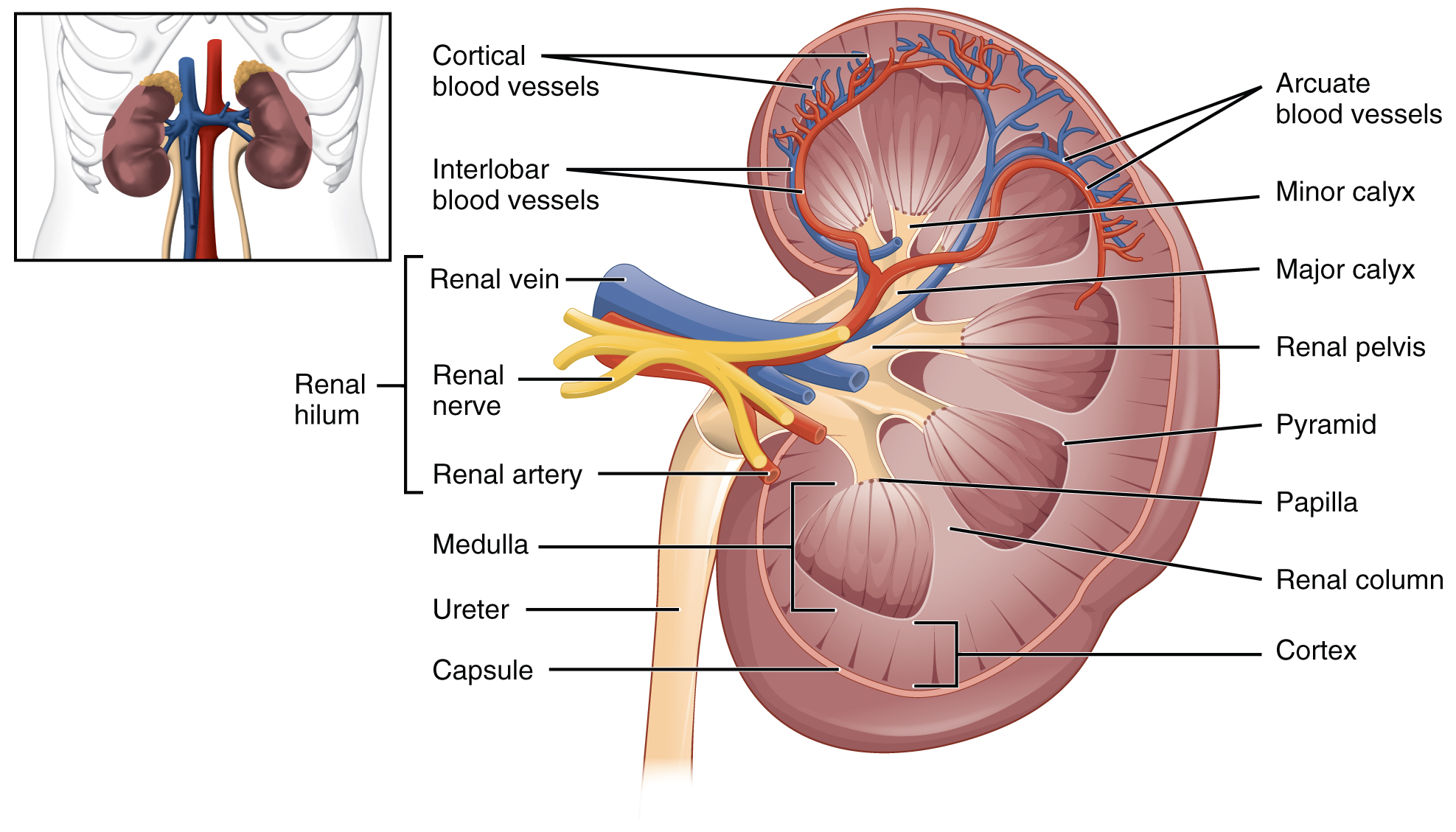
Renal Hilum
The renal hilum is the entry and exit site for structures servicing the kidneys: vessels, nerves, lymphatics, and ureters. The medial-facing hila are tucked into the sweeping convex outline of the cortex. Emerging from the hilum is the renal pelvis, which is formed from the major and minor calyxes in the kidney. The smooth muscle in the renal pelvis funnels urine via peristalsis into the ureter. The renal arteries form directly from the descending aorta, whereas the renal veins return cleansed blood directly to the inferior vena cava. The artery, vein, and renal pelvis are arranged in an anterior-to-posterior order.
Nephrons and Vessels
The renal artery first divides into segmental arteries, followed by further branching to form interlobar arteries that pass through the renal columns to reach the cortex (see Figure 8.3). The interlobar arteries, in turn, branch into arcuate arteries, cortical radiate arteries, and then into afferent arterioles. The afferent arterioles service about 1.3 million nephrons in each kidney.
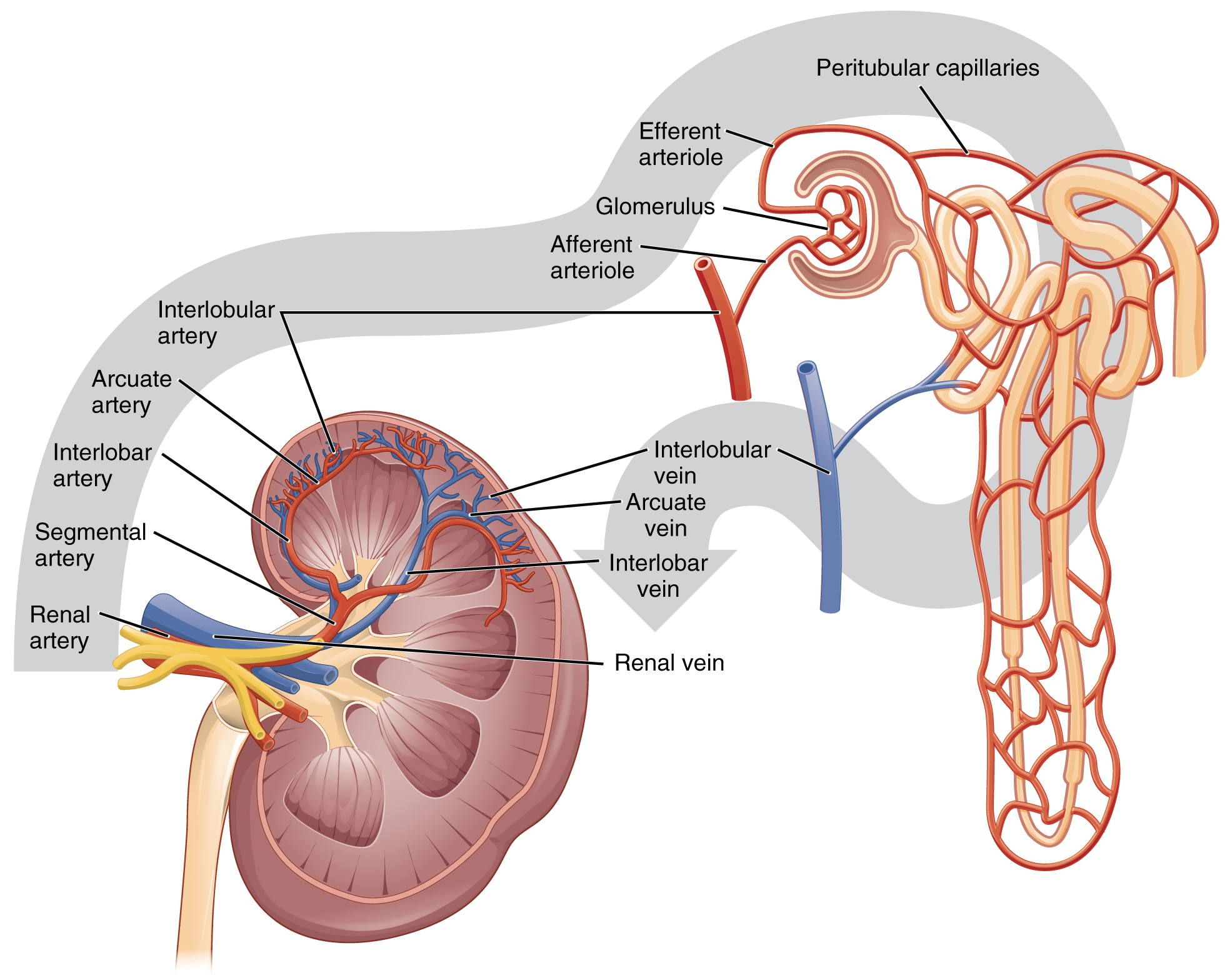
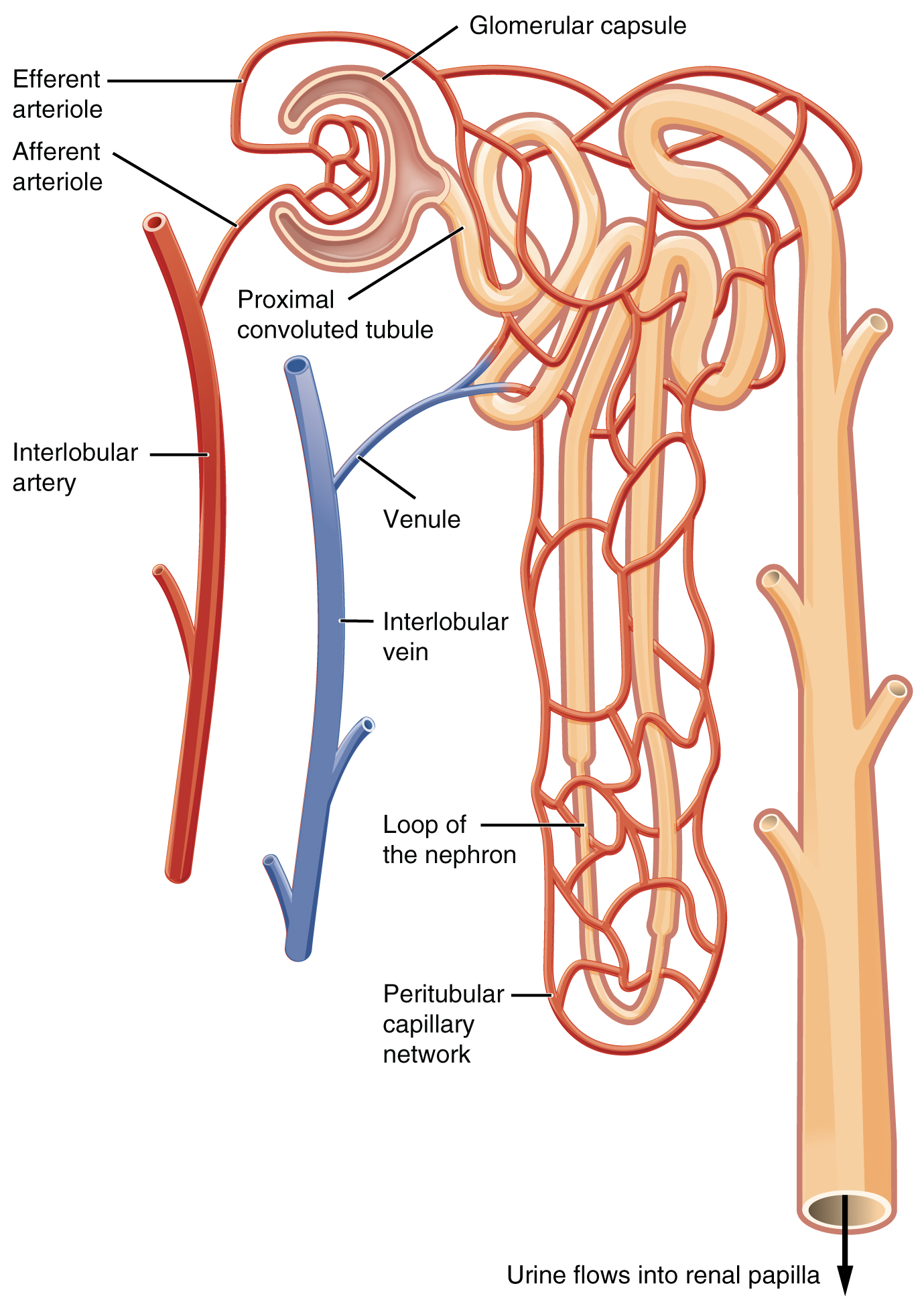
Nephrons are the “functional units” of the kidney; they cleanse the blood and balance the constituents of the circulation. The afferent arterioles form a tuft of high-pressure capillaries about 200 µm in diameter, the glomerulus. The rest of the nephron consists of a continuous sophisticated tubule whose proximal end surrounds the glomerulus in an intimate embrace—this is Bowman’s capsule. The glomerulus and Bowman’s capsule together form the renal corpuscle. As mentioned earlier, these glomerular capillaries filter the blood based on particle size. After passing through the renal corpuscle, the capillaries form a second arteriole, the efferent arteriole (see Figure 8.4). As the glomerular filtrate progresses through the nephron, these capillary networks recover most of the solutes and water, and return them to the circulation. Since a capillary bed (the glomerulus) drains into a vessel that in turn forms a second capillary bed, the definition of a portal system is met. This is the only portal system in which an arteriole is found between the first and second capillary beds. (Portal systems also link the hypothalamus to the anterior pituitary, and the blood vessels of the digestive viscera to the liver.
Ureter(s)
The kidneys and ureters are completely retroperitoneal, and the bladder has a peritoneal covering only over the dome. As urine is formed, it drains into the calyces of the kidney, which merge to form the funnel-shaped renal pelvis in the hilum of each kidney. The hilum narrows to become the ureter of each kidney. As urine passes through the ureter, it does not passively drain into the bladder but rather is propelled by waves of peristalsis. The ureters are approximately 30 cm long. The muscular layer of the ureter creates the peristaltic contractions to move the urine into the bladder without the aid of gravity.
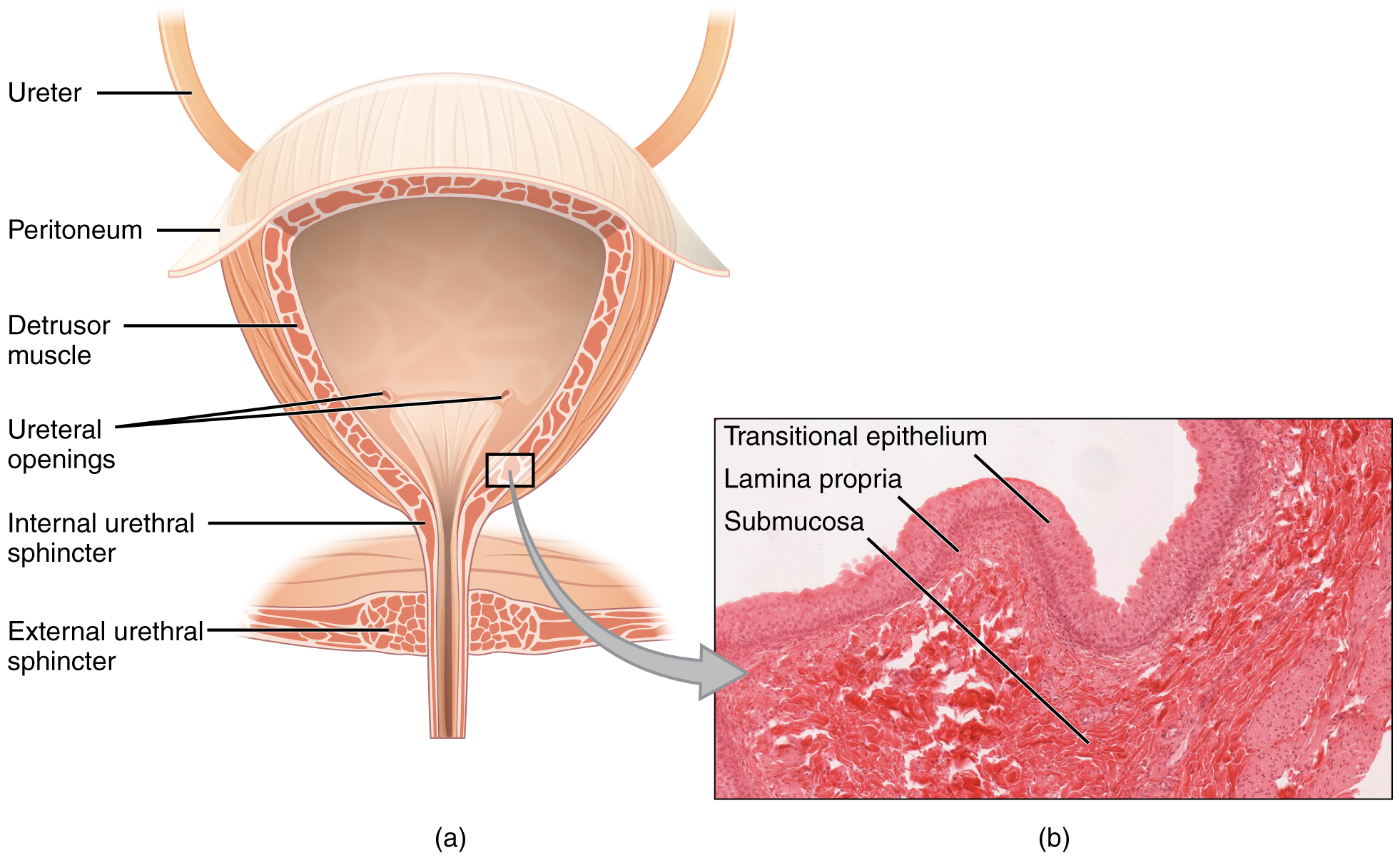
Bladder
The urinary bladder collects urine from both ureters ( see Figure 8.5). The bladder lies anterior to the uterus in females, posterior to the pubic bone and anterior to the rectum. During late pregnancy, its capacity is reduced due to compression by the enlarging uterus, resulting in increased frequency of urination. In males, the anatomy is similar, minus the uterus, and with the addition of the prostate inferior to the bladder. The bladder is partially retroperitoneal (outside the peritoneal cavity) with its peritoneal-covered “dome” projecting into the abdomen when the bladder is distended with urine.
Urethra
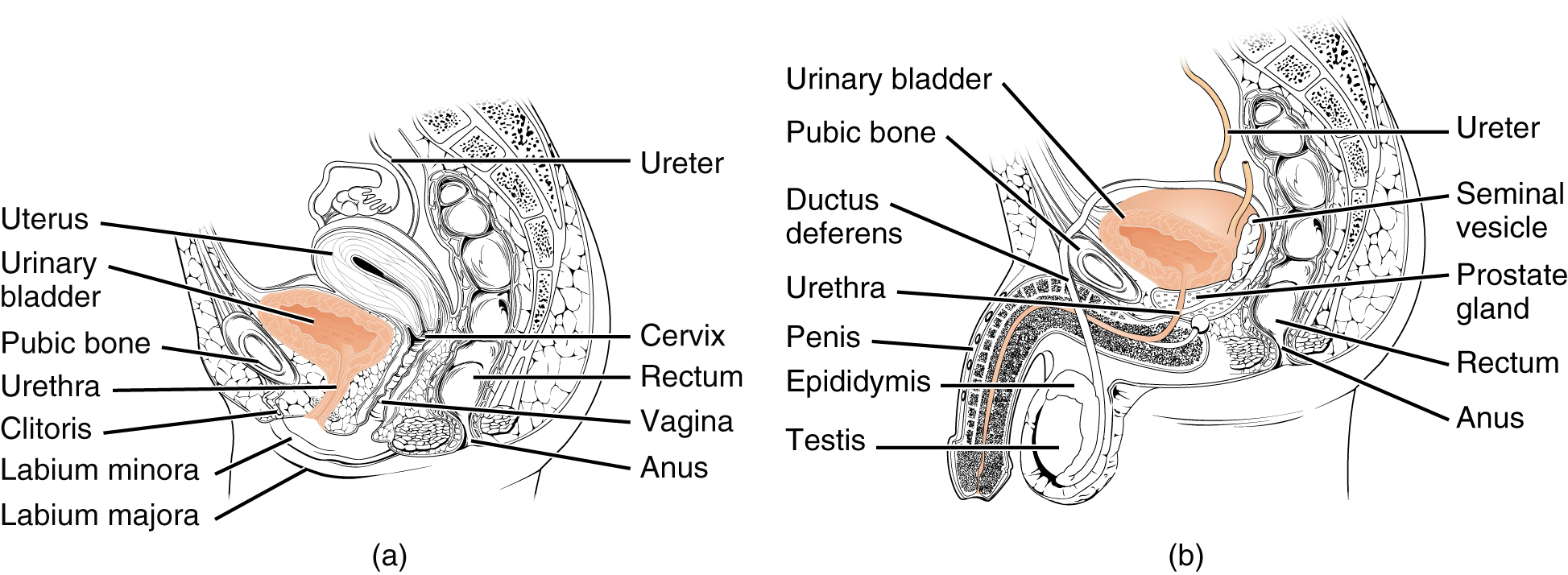
The urethra transports urine from the bladder to the outside of the body for disposal. The urethra is the only urologic organ that shows any significant anatomic difference between males and females; all other urine transport structures are identical (see Figure 8.6).
Voiding is regulated by an involuntary autonomic nervous system-controlled internal urinary sphincter, consisting of smooth muscle and voluntary skeletal muscle that forms the external urinary sphincter below it.
Micturition Reflex
Micturition is a less-often used, but proper term for urination or voiding. It results from an interplay of involuntary and voluntary actions by the internal and external urethral sphincters. When bladder volume reaches about 150 mL, an urge to void is sensed but is easily overridden. Voluntary control of urination relies on consciously preventing relaxation of the external urethral sphincter to maintain urinary continence. As the bladder fills, subsequent urges become harder to ignore. Ultimately, voluntary constraint fails with resulting incontinence, which will occur as bladder volume approaches 300 to 400 ml.
- Normal micturition is a result of stretch receptors in the bladder wall that transmit nerve impulses to the sacral region of the spinal cord to generate a spinal reflex. The resulting parasympathetic neural outflow causes contraction of the detrusor muscle and relaxation of the involuntary internal urethral sphincter.
- At the same time, the spinal cord inhibits somatic motor neurons, resulting in the relaxation of the skeletal muscle of the external urethral sphincter.
- The micturition reflex is active in infants but with maturity, children learn to override the reflex by asserting external sphincter control, thereby delaying voiding (potty training). This reflex may be preserved even in the face of spinal cord injury that results in paraplegia or quadriplegia. However, relaxation of the external sphincter may not be possible in all cases, and therefore, periodic catheterization may be necessary for bladder emptying.
Concept Check
- Describe two organs or structures essential to the urinary system.
- Identify the structure within the kidneys which filters blood.
- Name a commonly used term for the micturition reflex.
Anatomy Labeling Activity
Physiology (Function) of the Urinary System
- Remove waste products and medicines from the body
- Balance the body's fluids
- Balance a variety of electrolytes
- Release hormones to control blood pressure
- Release a hormone to control red blood cell production
- Help with bone health by controlling calcium and phosphorus
Having reviewed the anatomy of the urinary system now is the time to focus on physiology. You will discover that different parts of the nephron utilize specific processes to produce urine: filtration, reabsorption, and secretion. You will learn how each of these processes works and where they occur along the nephron and collecting ducts. The physiologic goal is to modify the composition of the plasma and, in doing so, produce the waste product urine.
Nephrons: The Functional Unit
Nephrons take a simple filtrate of the blood and modify it into urine. Many changes take place in the different parts of the nephron before urine is created for disposal. The term "forming urine" will be used hereafter to describe the filtrate as it is modified into true urine. The principal task of the nephron population is to balance the plasma to homeostatic set points and excrete potential toxins in the urine. They do this by accomplishing three principle functions—filtration, reabsorption, and secretion. They also have additional secondary functions that exert control in three areas: blood pressure (via the production of renin), red blood cell production (via the hormone EPO), and calcium absorption (via the conversion of calcidiol into calcitriol, the active form of vitamin D).
Loop of Henle
The descending and ascending portions of the loop of Henle (sometimes referred to as the nephron loop) are, of course, just continuations of the same tubule. They run adjacent and parallel to each other after having made a hairpin turn at the deepest point of their descent. The descending loop of Henle consists of an initial short, thick portion and long, thin portion, whereas the ascending loop consists of an initial short, thin portion followed by a long, thick portion. The descending and ascending thin portions consist of simple squamous epithelium. Different portions of the loop have different permeabilities for solutes and water.
Collecting Ducts
The collecting ducts are continuous with the nephron but are not technically part of it. In fact, each duct collects filtrate from several nephrons for final modification. Collecting ducts merge as they descend deeper in the medulla to form about 30 terminal ducts, which empty at a papilla.
Glomerular Filtration Rate (GFR)
The volume of filtrate formed by both kidneys per minute is termed the glomerular filtration rate (GFR). The heart pumps about 5 L blood per min under resting conditions. Approximately 20 percent or one liter enters the kidneys to be filtered. On average, this liter results in the production of about 125 mL/min filtrate produced in men (range of 90 to 140 mL/min) and 105 mL/min filtrate produced in women (range of 80 to 125 mL/min). This amount equates to a volume of about 180 L/day in men and 150 L/day in women. Ninety-nine percent of this filtrate is returned to the circulation by reabsorption so that only about 1–2 liters of urine are produced per day.
GFR is influenced by the hydrostatic pressure and colloid osmotic pressure on either side of the capillary membrane of the glomerulus. Recall that filtration occurs as pressure forces fluid and solutes through a semipermeable barrier with the solute movement constrained by particle size. Hydrostatic pressure is the pressure produced by a fluid against a surface. If you have fluid on both sides of a barrier, both fluids exert pressure in opposing directions. The net fluid movement will be in the direction of the lower pressure. Osmosis is the movement of solvent (water) across a membrane that is impermeable to a solute in the solution. This creates osmotic pressure which will exist until the solute concentration is the same on both sides of a semipermeable membrane. As long as the concentration differs, water will move. Glomerular filtration occurs when glomerular hydrostatic pressure exceeds the luminal hydrostatic pressure of Bowman’s capsule. There is also an opposing force, the osmotic pressure, which is typically higher in the glomerular capillary.
A proper concentration of solutes in the blood is important in maintaining osmotic pressure both in the glomerulus and systemically. There are disorders in which too much protein passes through the filtration slits into the kidney filtrate. This excess protein in the filtrate leads to a deficiency of circulating plasma proteins. In turn, the presence of protein in the urine allows it to hold more water in the filtrate and results in an increase in urine volume. Because there is less circulating protein, principally albumin, the osmotic pressure of the blood falls. Less osmotic pressure pulling water into the capillaries tips the balance towards hydrostatic pressure, which tends to push it out of the capillaries. The net effect is that water is lost from the circulation to interstitial tissues and cells. This “plumps up” the tissues and cells, a condition termed systemic edema.
Reabsorption and Secretion
The renal corpuscle filters the blood to create a filtrate that differs from blood mainly in the absence of cells and large proteins. From this point to the ends of the collecting ducts, the filtrate or forming urine is undergoing modification through secretion and reabsorption before true urine is produced. Here, some substances are reabsorbed, whereas others are secreted. Note the use of the term “reabsorbed.” All of these substances were “absorbed” in the digestive tract—99 percent of the water and most of the solutes filtered by the nephron must be reabsorbed. Water and substances that are reabsorbed are returned to the circulation by the peritubular and vasa recta capillaries.
Urinalysis
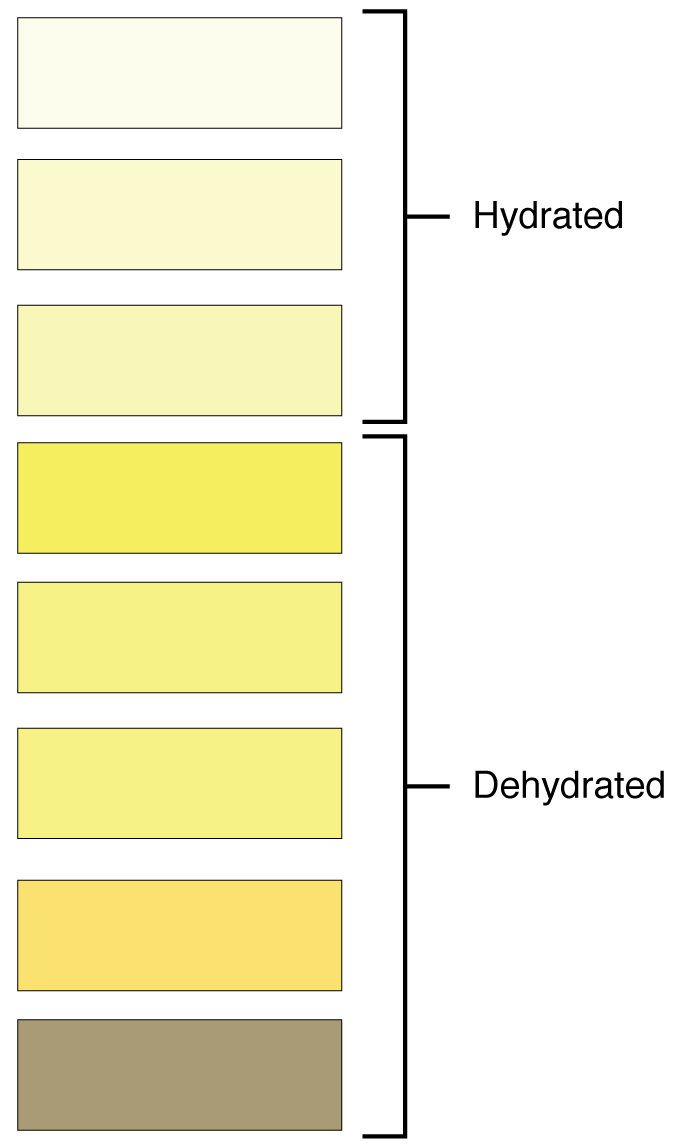
Urinalysis (urine analysis) often provides clues to renal disease. Normally, only traces of protein are found in urine, and when higher amounts are found, damage to the glomeruli is the likely basis. Unusually large quantities of urine may point to diseases like diabetes mellitus or hypothalamic tumors that cause diabetes insipidus. The color of urine is determined mostly by the breakdown products of red blood cell destruction (see Figure 8.8). The “heme” of hemoglobin is converted by the liver into water-soluble forms that can be excreted into the bile and indirectly into the urine. This yellow pigment is urochrome. Urine color may also be affected by certain foods like beets, berries, and fava beans. A kidney stone or a cancer of the urinary system may produce sufficient bleeding to manifest as pink or even bright red urine. Diseases of the liver or obstructions of bile drainage from the liver impart a dark “tea” or “cola” hue to the urine. Dehydration produces darker, concentrated urine that may also possess the slight odor of ammonia. Most of the ammonia produced from protein breakdown is converted into urea by the liver, so ammonia is rarely detected in fresh urine. The strong ammonia odor you may detect in bathrooms or alleys is due to the breakdown of urea into ammonia by bacteria in the environment. About one in five people detect a distinctive odor in their urine after consuming asparagus; other foods such as onions, garlic, and fish can impart their own aromas! These food-caused odors are harmless.
Urine volume varies considerably. The normal range is one to two liters per day. The kidneys must produce a minimum urine volume of about 500 mL/day to rid the body of wastes. Output below this level may be caused by severe dehydration or renal disease and is termed oliguria. The virtual absence of urine production is termed anuria. Excessive urine production is polyuria, which may be due to diabetes mellitus or diabetes insipidus. In diabetes mellitus, blood glucose levels exceed the number of available sodium-glucose transporters in the kidney, and glucose appears in the urine. The osmotic nature of glucose attracts water, leading to its loss in the urine. In the case of diabetes insipidus, insufficient pituitary antidiuretic hormone (ADH) release or insufficient numbers of ADH receptors in the collecting ducts means that too few water channels are inserted into the cell membranes that line the collecting ducts of the kidney. Insufficient numbers of water channels (aquaporins) reduce water absorption, resulting in high volumes of very dilute urine.
Concept Check
- Contrast the following terms: oliguria, anuria and polyuria. What are the differences between these terms as they describe urinary output?
- Explain how urine colour varies based on food consumed and/or hydration levels.
Endocrine Urinary Function
Several hormones have specific, important roles in regulating kidney function. They act to stimulate or inhibit blood flow. Some of these are endocrine, acting from a distance, whereas others are paracrine, acting locally.
Renin–Angiotensin–Aldosterone
Renin is an enzyme that is produced by the granular cells of the afferent arteriole. It enzymatically converts angiotensinogen (made by the liver, freely circulating) into angiotensin I. Its release is stimulated by prostaglandins to decreased extracellular fluid volume.
Angiotensin II is a potent vasoconstrictor that plays an immediate role in the regulation of blood pressure. It acts systemically to cause vasoconstriction as well as constriction of both the afferent and efferent arterioles of the glomerulus. In instances of blood loss or dehydration, it reduces both GFR and renal blood flow, thereby limiting fluid loss and preserving blood volume. Its release is usually stimulated by decreases in blood pressure, and so the preservation of adequate blood pressure is its primary role.
Aldosterone is often called the “salt-retaining hormone,” is released from the adrenal cortex in response to angiotensin II or directly in response to increased plasma potassium. It promotes sodium reabsorption by the nephron, promoting the retention of water.
Antidiuretic Hormone (ADH)
Diuretics are drugs that can increase water loss by interfering with the recapture of solutes and water from the forming urine. They are often prescribed to lower blood pressure. Coffee, tea, and alcoholic beverages are familiar diuretics. ADH, released by the posterior pituitary, works to do the exact opposite. It promotes the recovery of water, decreases urine volume, and maintains plasma osmolarity and blood pressure. It does so by stimulating the movement of aquaporin proteins into the apical cell membrane of principal cells of the collecting ducts to form water channels, allowing the transcellular movement of water from the lumen of the collecting duct into the interstitial space in the medulla of the kidney by osmosis. From there, it enters the vasa recta capillaries to return to the circulation. Water is attracted by the high osmotic environment of the deep kidney medulla.
Parathyroid Hormone
Parathyroid hormone (PTH) is produced by the parathyroid glands in response to decreased circulating calcium levels.
Maintaining Homeostasis
Homeostasis requires that volume and osmolarity be preserved. Blood volume is important in maintaining sufficient blood pressure, and there are nonrenal mechanisms involved in its preservation, including vasoconstriction, which can act within seconds of a drop in pressure. Thirst mechanisms are also activated to promote the consumption of water lost through respiration, evaporation, or urination. Hormonal mechanisms are activated to recover volume while maintaining a normal osmotic environment. These mechanisms act principally on the kidney.
Diuretics and Fluid Volume
A diuretic is a compound that increases urine volume. Three familiar drinks contain diuretic compounds: coffee, tea, and alcohol. The caffeine in coffee and tea works by promoting vasodilation in the nephron, which increases GFR. Alcohol increases GFR by inhibiting ADH release from the posterior pituitary, resulting in less water recovery by the collecting duct. In cases of high blood pressure, diuretics may be prescribed to reduce blood volume and, thereby, reduce blood pressure. The most frequently prescribed anti-hypertensive diuretic is hydrochlorothiazide.
Regulation of Nitrogen Wastes
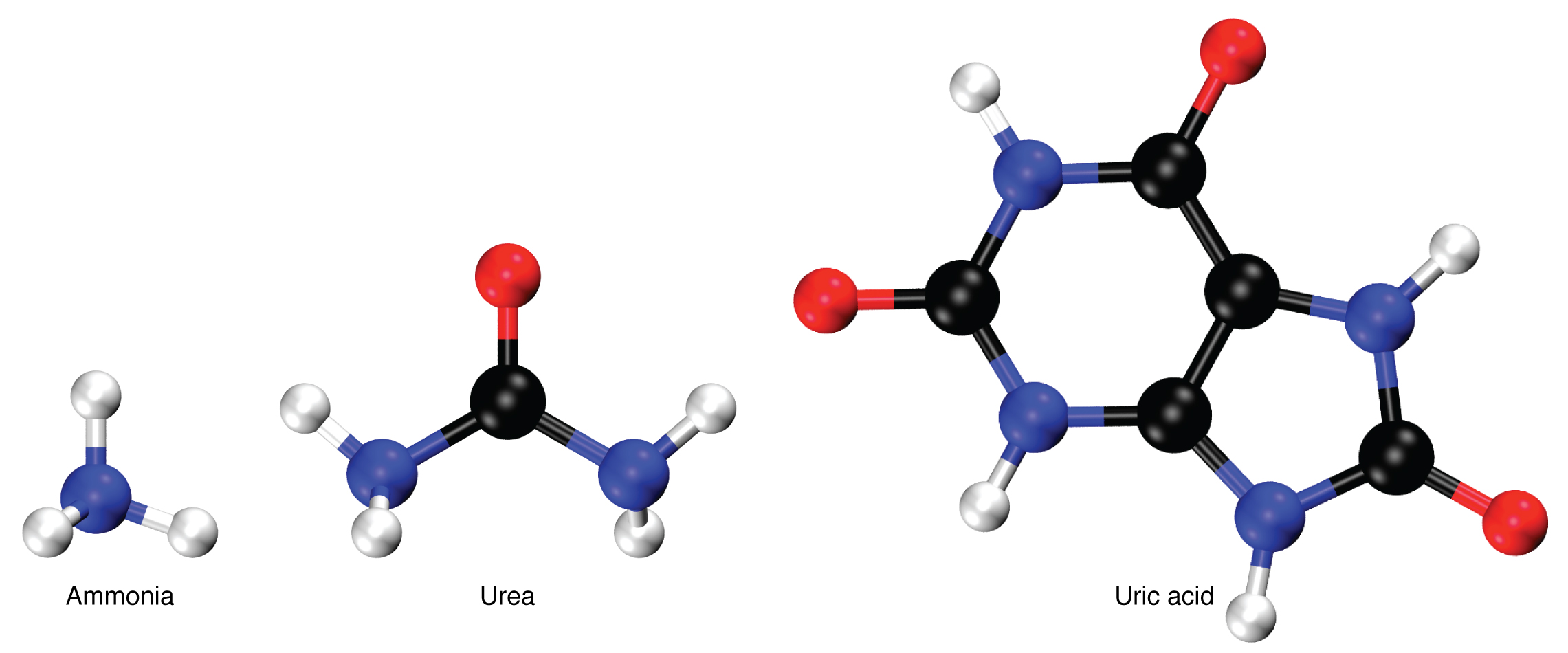
Nitrogen wastes are produced by the breakdown of proteins during normal metabolism. Proteins are broken down into amino acids, which in turn are deaminated by having their nitrogen groups removed. Deamination converts the amino (NH2) groups into ammonia (NH3), ammonium ion (NH4+), urea, or uric acid (Figure 8.9). Ammonia is extremely toxic, so most of it is very rapidly converted into urea in the liver. Human urinary wastes typically contain primarily urea with small amounts of ammonium and very little uric acid.
Elimination of Drugs and Hormones
Water-soluble drugs may be excreted in the urine and are influenced by one or all of the following processes: glomerular filtration, tubular secretion, or tubular reabsorption. Drugs that are structurally small can be filtered by the glomerulus with the filtrate. Large drug molecules such as heparin or those that are bound to plasma proteins cannot be filtered and are not readily eliminated. Some drugs can be eliminated by carrier proteins that enable secretion of the drug into the tubule lumen. There are specific carriers that eliminate basic (such as dopamine or histamine) or acidic drugs (such as penicillin or indomethacin). As is the case with other substances, drugs may be both filtered and reabsorbed passively along a concentration gradient.
Watch this video:
Media 8.2. Urinary System, Part 2: Crash Course A&P #39 [Online video]. Copyright 2015 by CrashCourse.
Urinary System Medical Terms not Easily Broken into Word Parts
Urinary System Abbreviations
Many terms and phrases related to the urinary system are abbreviated.
Learn these common abbreviations by expanding the list below.
Diseases and Disorders
Diabetic Nephropathy
Diabetic nephropathy impacts the kidneys as a result of having diabetes mellitus type 1 or 2. Higher levels of blood sugar can lead to high blood pressure and this additional pressure exerted on the kidneys causes destruction of the small filtering structures within the kidney. (Mayo Clinic Staff, 2019). To learn more about diabetic nephropathy visit the Mayo Clinic's Diabetic Nephropathy web page.
Glomerulonephritis
Glomerulonephritis refers to acute or chronic nephritis that involves inflammation of the capillaries of the renal glomeruli. It has various causes, and is noted especially by blood or protein in the urine and by edema. If untreated, it could lead to kidney failure.
Hydronephrosis
Hydronephrosis is a condition whereby the kidneys begin to swell because of the retention of urine. Several conditions can cause hydronephrosis, such as a kidney stone or blood clot. Treatment will vary, depending on the cause (Cleveland Clinic, 2019). To learn more about hydronephrosis the Cleveland Clinic's web page on hydronephrosis.
Polycystic Kidney Disease
Polycystic kidney disease (PKD) is a genetic disease where cysts grow inside the kidneys. The kidneys enlarge from the cystic collections and damage to the filtering structures of the kidneys can occur. As the disease progresses it may lead to chronic kidney disease (American Kidney Fund, 2020). To learn more, visit the Kidney Fund's PKD web page.
Renal Cell Carcinoma
Renal cell carcinoma is a cancer occurring in the kidney tubes where urine is produced or collected. This one of the most common cancers found within the kidneys. Removal of the cancerous lesions is the typical approach from a treatment perspective (Innovation for Patient Care, 2018). To learn more, visit Innovation for Patient Care's web page on renal cell carcinoma.
Renal Failure
Renal failure occurs when kidneys suddenly or gradually become unable to filter waste products from blood. When kidneys stop filtering, high level of wastes may build. Two types exist acute kidney failure and chronic kidney failure (Mayo Clinic Staff, 2019a). To learn more about kidney failure visit the Mayo Clinic's page on Chronic Kidney Failure.
Cystitis
Cystitis is inflammation of the urinary bladder, often caused by an infection. A chronic form of this condition is known as interstitial cystitis. Symptoms of cystitis include bladder pressure, voiding frequently, and pain (Mayo Clinic Staff, 2019b). To learn more about cystitis visit the Mayo Clinic's page on Interstitial Cystitis.
Urinary Tract Infection
A urinary tract infection (UTI) is an infection caused by bacteria, or sometimes, fungi. The exact type of bacterial growth is determined by conducting urine for culture and sensitivity (C&S) testing. In rare cases a UTI may be caused by a virus (Lights & Boskey, 2019). For more information, visit Healthline's web page on Urinary Tract Infections.
Urinary Incontinence
Urinary incontinence is a loss of bladder control. Those afflicted with the condition will experience urine leakage from the bladder. Weak bladder muscles are a risk factor for developing this condition (Kim & O'Connell, 2017). To learn more about this condition visit Healthline's webpage Urologic Diseases.
Medical Terms in Context
Medical Specialties and Procedures Related to the Urinary System
Urology is specialty that "addresses the medical and surgical treatment of disorders and diseases of the female urinary tract and the male urogenital system" (Canadian Medical Association, 2018). This specialty focuses on diagnosis, treatment, and surgical repair. Common clinical visits involve kidney stones, kidney failure and bladder dysfunction. To learn more about urology as a specialty visit the Urology Profile (PDF file) authored by the Canadian Medical Association.
Urologist
A urologist is a medical specialist involved in the diagnosis and treatment of urinary and male genitourinary system conditions, disorders, and diseases such as prostate disease, renal and bladder dysfunctions, and others (Canadian Medical Association, 2018).
Procedures and Testing
Urinalysis
A urinalysis is microscopic group of urine testing. This test detects and measures several substances in the urine such as products of normal and abnormal metabolism and bacteria (Lab Tests Online, 2020). To learn more about urinalysis visit Lab Tests Online's Urinalysis web page.
Urine for C&S
Urine for culture and sensitivity. Urine produced by the kidneys is analyzed by way of a urine culture test which can detect and identify bacteria in the urine, which may be causing a urinary tract infection (UTI). If harmful bacteria is found a sensitivity report is generated. This report lists antibiotics sensitive in the treatment of the bacteria present (Lab Tests Online, 2020a). To learn more about Urine for C&S, visit Lab Tests Online's Urine Culture web page.
24 Hour Urine Collection
This is a test whereby all urinary output is collected over a 24-hour period of time. The analysis of urinary output over this extended period of time provides a greater indication of normal or abnormal kidney function (Lab Tests Online, 2017). To learn more a, visit Lab Tests Online's 24-hour Urine Sample article.
CT Scan of Kidney
Computed tomography is a diagnostic imaging procedure that uses a combination of x-rays and computer technology to produce a variety of images. It provides detailed images of the kidney looking for disease, cancer, obstructions and other kidney conditions (Johns Hopkins Medicine, n.d.) . To learn more about a CT scan of the kidney visit Johns Hopkins Medicine's page on Computed Tomography (CT or CAT) Scan of the Kidney.
Cystoscopy
A cystoscopy is a procedure allowing a physician to check for bladder or ureteral problems, such as bladder cancer. An endoscope, also known as a cystoscope, containing a camera at the end of it is used (Canadian Cancer Society, 2020). To learn more about cystoscopy visit the Canadian Cancer Society's Cystoscopy and Ureteroscopy web page .
Dialysis
Dialysis is a treatment that removes waste products from the blood when the kidneys are not fully functioning. This type of therapy is available at home or in a hospital or clinic and there are two main types: peritoneal dialysis and hemodialysis (Kidney Foundation, 2020). To learn more about dialysis visit the Kidney Foundation's Dialysis web page.
Intravenous Pyelogram
An intravenous pyelogram (IVP) is a specialized x-ray designed to produce views of the entire urinary tract. A dye is used to secure the enhanced imaging. The x-rays can also show how well the urinary tract is functioning and any identify any blockages (Canadian Cancer Society, 2020a). To learn more about IVP visit the Canadian Cancer Society's IVP web page.
Kidney Scan
A kidney scan is an imaging test which views the kidneys. It is considered a nuclear imaging test as it uses radioactive tracers to pick up hot or cold spots within the kidney. These variation are are considered abnormal.
Kidney Transplant
When kidneys fail or when a person is in end stage chronic kidney disease, a surgical procedure is performed in the form of a kidney transplant. This procedure involves harvesting a donor kidney which is transplanted into the recipient in need of a functioning kidney to support vital function of the urinary system.
Urinary System Vocabulary
Adventitial
The outermost layer of the wall of a blood vessel.
Apical
Relating to or denoting an apex.
Autonomic
Involuntary or unconscious.
Calyces
A cuplike cavity or structure.
Deamination
The removal of an amino group from a molecule.
Detrusor
A muscle which forms a layer of the wall of the bladder.
Excretion
Waste is eliminated from an organism. In vertebrates this is primarily carried out by the lungs, kidneys and skin.
Homeostasis
A biological process that results in stable equilibrium.
Hydrostatic
Relating to the equilibrium of liquids and the pressure exerted by liquid at rest.
Hypothalmic
A region of the forebrain below the thalamus.
Lethargy
Periods of weakness.
Mitochondria
An organelle found in large numbers in most cells.
Osmosis
A process by which molecules of a solvent tend to pass through a membrane from a less concentrated solution into a more concentrated one.
pH
pH is a measure of how acidic or alkaline a substance is, as determined by the number of free hydrogen ions in the substance.
Prostaglandins
Any of a group of compounds with varying hormone-like effects.
Pseudostratified
Consisting of closely packed cells which appear to be arranged in layers.
Solutes
The minor component in a solution.
Voiding
Excrete (waste matter).
Test Yourself
References
American Kidney Fund. (2020, June 17). Polycystic kidney disease. https://www.kidneyfund.org/kidney-disease/other-kidney-conditions/polycystic-kidney-disease.html
Canadian Medical Association. (2018, August). Urology profile. Canadian Medical Association Speciatly Profiles. https://www.cma.ca/sites/default/files/2019-01/urology-e.pdf
Canadian Cancer Society. (2020). Cystoscopy and ureteroscopy. Canadian Cancer Society: Cancer Information. https://www.cancer.ca/en/cancer-information/diagnosis-and-treatment/tests-and-procedures/cystoscopy/?region=on
Canadian Cancer Society. (2020a). Intravenous pyelogram. Canadian Cancer Society: Cancer Information. https://www.cancer.ca/en/cancer-information/diagnosis-and-treatment/tests-and-procedures/intravenous-pyelogram/?region=on
Cleveland Clinic. (2019, May 22). Hydronephrosis. https://my.clevelandclinic.org/health/diseases/15417-hydronephrosis
[CrashCourse]. (2015, October 12). Urinary system, part 1: Crash course A&P #38 [Video]. YouTube. https://www.youtube.com/watch?v=l128tW1H5a8
[CrashCourse]. (2015, June 22). Urinary system, part 2: Crash course A&P #39 [Video]. YouTube. https://youtu.be/DlqyyyvTI3k
Innovation for Patient Care. (2020, October 16). Renal cell carcinoma: The most common form of kidney cancer in adults. https://www.ipsen.ca/therapeutic-areas/oncology/renal-cell-carcinoma/
Johns Hopkins Medicine. (n.d.). Computed tomography (CT or CAT) scan of the kidney. John Hopkins Medicine: Health. https://www.hopkinsmedicine.org/health/treatment-tests-and-therapies/ct-scan-of-the-kidney
Kidney Foundation of Canada. (2020). Dialysis. Kidney Foundation. https://kidney.ca/Kidney-Health/Living-With-Kidney-Failure/Dialysis
Lab Tests Online. (2017, July 10). 24-hour urine sample. https://labtestsonline.org/glossary/urine-24
Lab Tests Online. (2020, June 16). Urinalysis. https://labtestsonline.org/tests/urinalysis
Lab Tests Online. (2020a, January 30). Urine culture. https://labtestsonline.org/tests/urinalysis
Lights, V., & Boskey, E. (2019, March 21). Everything you need to know about urinary tract infection. Healthline. https://www.healthline.com/health/urinary-tract-infection-adults
Mayo Clinic Staff. (2019a, August 15). Chronic kidney disease. Mayo Clinic. https://www.mayoclinic.org/diseases-conditions/chronic-kidney-disease/symptoms-causes/syc-20354521
Mayo Clinic Staff. (2019, September 19). Diabetic nephropathy. Mayo Clinic. https://www.mayoclinic.org/diseases-conditions/diabetic-nephropathy/symptoms-causes/syc-20354556
Mayo Clinic Staff. (2019b, September 14). Interstitial cystitis. Mayo Clinic. https://www.mayoclinic.org/diseases-conditions/interstitial-cystitis/symptoms-causes/syc-20354357
Image Descriptions
Figure 8.2 image description: LeftThe left panel of this figure shows the location of the kidneys in the abdomen. The right panel shows the cross section of the kidney. [Return to Figure 8.2].
Figure 8.5 image description: The left panel of this figure shows the cross section of the bladder and the major parts are labeled. The right panel shows a micrograph of the bladder. [Return to Figure 8.5].
Figure 8.6 image description: Diagrams of the (a) female and (b) male genitalia highlighting the respective urethras. [Return to Figure 8.6].
Figure 8.7 image description: This figure shows the different pressures acting across the glomerulus including blood hydrostatic pressure, blood colloid osmotic pressure, capsular hydrostatic pressure. [Return to Figure 8.7].
Figure 8.8 image description: This color chart shows 8 different shades of yellow and associates each shade with stages of hydration (lightest 3 shades) or dehydration (remaining 5 darker shades). [Return to Figure 8.8].
Unless otherwise indicated, this chapter contains material adapted from Anatomy and Physiology (on OpenStax), by Betts, et al. and is used under a a CC BY 4.0 international license. Download and access this book for free at https://openstax.org/books/anatomy-and-physiology/pages/1-introduction.
fat cells
Cells that engulf and absorb bacteria and cell particles
Tactile corpsucle that responds to light and touch, touch receptors.
net like
fibrous tissue
WTCS Learning Objectives
- Apply the rules of medical language to build, analyze, spell, pronounce, abbreviate, and define terms as they relate to the urinary system
- Identify meanings of key word components of the urinary system
- Categorize diagnostic, therapeutic, procedural or anatomic terms related to the urinary system
- Use terms related to the urinary system
- Use terms related to the diseases and disorders of the urinary system
Urinary System Word Parts
Click on prefixes, combining forms, and suffixes to reveal a list of word parts to memorize for the urinary system. Then use the flashcards below to practice.
Introduction to the Urinary System
The urinary system has roles you may be well aware of. Cleansing the blood and ridding the body of wastes probably come to mind. However, there are additional, equally important functions, played by the system. Take, for example, regulation of pH, a function shared with the lungs and the buffers in the blood. Additionally, the regulation of blood pressure is a role shared with the heart and blood vessels. What about regulating the concentration of solutes in the blood? Did you know that the kidney is important in determining the concentration of red blood cells? Eighty-five percent of the erythropoietin (EPO) produced to stimulate red blood cell production is produced in the kidneys. The kidneys also help control blood pressure by producing the enzyme renin . Additionally, the kidneys perform the final synthesis step of vitamin D production, converting calcidiol to calcitriol, the active form of vitamin D. If the kidneys fail, these functions are compromised or lost altogether, with devastating effects on homeostasis.
Watch this video:
Media 8.1. Urinary System, Part 1: Crash Course A&P #38 [Online video]. Copyright 2015 by CrashCourse.
Urinary System Medical Terms
Anatomy (Structures) of the Urinary System
Kidney(s)
The kidneys lie on either side of the spine in the retroperitoneal space between the parietal peritoneum and the posterior abdominal wall, well protected by muscle, fat, and ribs. They are roughly the size of your fist. The male kidney is typically a bit larger than the female kidney. The kidneys are well vascularized, receiving about twenty-five percent of the cardiac output at rest. Figure 8.1 displays the location of the kidneys.
Kidneys' Internal Structure
A frontal section through the kidney reveals an outer region called the renal cortex and an inner region called the medulla (see Figure 8.2). The renal columns are connective tissue extensions that radiate downward from the cortex through the medulla to separate the most characteristic features of the medulla, the renal pyramids and renal papillae. The papillae are bundles of collecting ducts that transport urine made by nephrons to the calyces of the kidney for excretion. The renal columns also serve to divide the kidney into 6–8 lobes and provide a supportive framework for vessels that enter and exit the cortex. The pyramids and renal columns taken together constitute the kidney lobes.
Renal Hilum
The renal hilum is the entry and exit site for structures servicing the kidneys: vessels, nerves, lymphatics, and ureters. The medial-facing hila are tucked into the sweeping convex outline of the cortex. Emerging from the hilum is the renal pelvis, which is formed from the major and minor calyxes in the kidney. The smooth muscle in the renal pelvis funnels urine via peristalsis into the ureter. The renal arteries form directly from the descending aorta, whereas the renal veins return cleansed blood directly to the inferior vena cava. The artery, vein, and renal pelvis are arranged in an anterior-to-posterior order.
Nephrons and Vessels
The renal artery first divides into segmental arteries, followed by further branching to form interlobar arteries that pass through the renal columns to reach the cortex (see Figure 8.3). The interlobar arteries, in turn, branch into arcuate arteries, cortical radiate arteries, and then into afferent arterioles. The afferent arterioles service about 1.3 million nephrons in each kidney.
Nephrons are the “functional units” of the kidney; they cleanse the blood and balance the constituents of the circulation. The afferent arterioles form a tuft of high-pressure capillaries about 200 µm in diameter, the glomerulus. The rest of the nephron consists of a continuous sophisticated tubule whose proximal end surrounds the glomerulus in an intimate embrace—this is Bowman’s capsule. The glomerulus and Bowman’s capsule together form the renal corpuscle. As mentioned earlier, these glomerular capillaries filter the blood based on particle size. After passing through the renal corpuscle, the capillaries form a second arteriole, the efferent arteriole (see Figure 8.4). As the glomerular filtrate progresses through the nephron, these capillary networks recover most of the solutes and water, and return them to the circulation. Since a capillary bed (the glomerulus) drains into a vessel that in turn forms a second capillary bed, the definition of a portal system is met. This is the only portal system in which an arteriole is found between the first and second capillary beds. (Portal systems also link the hypothalamus to the anterior pituitary, and the blood vessels of the digestive viscera to the liver.
Ureter(s)
The kidneys and ureters are completely retroperitoneal, and the bladder has a peritoneal covering only over the dome. As urine is formed, it drains into the calyces of the kidney, which merge to form the funnel-shaped renal pelvis in the hilum of each kidney. The hilum narrows to become the ureter of each kidney. As urine passes through the ureter, it does not passively drain into the bladder but rather is propelled by waves of peristalsis. The ureters are approximately 30 cm long. The muscular layer of the ureter creates the peristaltic contractions to move the urine into the bladder without the aid of gravity.
Bladder
The urinary bladder collects urine from both ureters ( see Figure 8.5). The bladder lies anterior to the uterus in females, posterior to the pubic bone and anterior to the rectum. During late pregnancy, its capacity is reduced due to compression by the enlarging uterus, resulting in increased frequency of urination. In males, the anatomy is similar, minus the uterus, and with the addition of the prostate inferior to the bladder. The bladder is partially retroperitoneal (outside the peritoneal cavity) with its peritoneal-covered “dome” projecting into the abdomen when the bladder is distended with urine.
Urethra
The urethra transports urine from the bladder to the outside of the body for disposal. The urethra is the only urologic organ that shows any significant anatomic difference between males and females; all other urine transport structures are identical (see Figure 8.6).
Voiding is regulated by an involuntary autonomic nervous system-controlled internal urinary sphincter, consisting of smooth muscle and voluntary skeletal muscle that forms the external urinary sphincter below it.
Micturition Reflex
Micturition is a less-often used, but proper term for urination or voiding. It results from an interplay of involuntary and voluntary actions by the internal and external urethral sphincters. When bladder volume reaches about 150 mL, an urge to void is sensed but is easily overridden. Voluntary control of urination relies on consciously preventing relaxation of the external urethral sphincter to maintain urinary continence. As the bladder fills, subsequent urges become harder to ignore. Ultimately, voluntary constraint fails with resulting incontinence, which will occur as bladder volume approaches 300 to 400 ml.
- Normal micturition is a result of stretch receptors in the bladder wall that transmit nerve impulses to the sacral region of the spinal cord to generate a spinal reflex. The resulting parasympathetic neural outflow causes contraction of the detrusor muscle and relaxation of the involuntary internal urethral sphincter.
- At the same time, the spinal cord inhibits somatic motor neurons, resulting in the relaxation of the skeletal muscle of the external urethral sphincter.
- The micturition reflex is active in infants but with maturity, children learn to override the reflex by asserting external sphincter control, thereby delaying voiding (potty training). This reflex may be preserved even in the face of spinal cord injury that results in paraplegia or quadriplegia. However, relaxation of the external sphincter may not be possible in all cases, and therefore, periodic catheterization may be necessary for bladder emptying.
Concept Check
- Describe two organs or structures essential to the urinary system.
- Identify the structure within the kidneys which filters blood.
- Name a commonly used term for the micturition reflex.
Anatomy Labeling Activity
Physiology (Function) of the Urinary System
- Remove waste products and medicines from the body
- Balance the body's fluids
- Balance a variety of electrolytes
- Release hormones to control blood pressure
- Release a hormone to control red blood cell production
- Help with bone health by controlling calcium and phosphorus
Having reviewed the anatomy of the urinary system now is the time to focus on physiology. You will discover that different parts of the nephron utilize specific processes to produce urine: filtration, reabsorption, and secretion. You will learn how each of these processes works and where they occur along the nephron and collecting ducts. The physiologic goal is to modify the composition of the plasma and, in doing so, produce the waste product urine.
Nephrons: The Functional Unit
Nephrons take a simple filtrate of the blood and modify it into urine. Many changes take place in the different parts of the nephron before urine is created for disposal. The term "forming urine" will be used hereafter to describe the filtrate as it is modified into true urine. The principal task of the nephron population is to balance the plasma to homeostatic set points and excrete potential toxins in the urine. They do this by accomplishing three principle functions—filtration, reabsorption, and secretion. They also have additional secondary functions that exert control in three areas: blood pressure (via the production of renin), red blood cell production (via the hormone EPO), and calcium absorption (via the conversion of calcidiol into calcitriol, the active form of vitamin D).
Loop of Henle
The descending and ascending portions of the loop of Henle (sometimes referred to as the nephron loop) are, of course, just continuations of the same tubule. They run adjacent and parallel to each other after having made a hairpin turn at the deepest point of their descent. The descending loop of Henle consists of an initial short, thick portion and long, thin portion, whereas the ascending loop consists of an initial short, thin portion followed by a long, thick portion. The descending and ascending thin portions consist of simple squamous epithelium. Different portions of the loop have different permeabilities for solutes and water.
Collecting Ducts
The collecting ducts are continuous with the nephron but are not technically part of it. In fact, each duct collects filtrate from several nephrons for final modification. Collecting ducts merge as they descend deeper in the medulla to form about 30 terminal ducts, which empty at a papilla.
Glomerular Filtration Rate (GFR)
The volume of filtrate formed by both kidneys per minute is termed the glomerular filtration rate (GFR). The heart pumps about 5 L blood per min under resting conditions. Approximately 20 percent or one liter enters the kidneys to be filtered. On average, this liter results in the production of about 125 mL/min filtrate produced in men (range of 90 to 140 mL/min) and 105 mL/min filtrate produced in women (range of 80 to 125 mL/min). This amount equates to a volume of about 180 L/day in men and 150 L/day in women. Ninety-nine percent of this filtrate is returned to the circulation by reabsorption so that only about 1–2 liters of urine are produced per day.
GFR is influenced by the hydrostatic pressure and colloid osmotic pressure on either side of the capillary membrane of the glomerulus. Recall that filtration occurs as pressure forces fluid and solutes through a semipermeable barrier with the solute movement constrained by particle size. Hydrostatic pressure is the pressure produced by a fluid against a surface. If you have fluid on both sides of a barrier, both fluids exert pressure in opposing directions. The net fluid movement will be in the direction of the lower pressure. Osmosis is the movement of solvent (water) across a membrane that is impermeable to a solute in the solution. This creates osmotic pressure which will exist until the solute concentration is the same on both sides of a semipermeable membrane. As long as the concentration differs, water will move. Glomerular filtration occurs when glomerular hydrostatic pressure exceeds the luminal hydrostatic pressure of Bowman’s capsule. There is also an opposing force, the osmotic pressure, which is typically higher in the glomerular capillary.
A proper concentration of solutes in the blood is important in maintaining osmotic pressure both in the glomerulus and systemically. There are disorders in which too much protein passes through the filtration slits into the kidney filtrate. This excess protein in the filtrate leads to a deficiency of circulating plasma proteins. In turn, the presence of protein in the urine allows it to hold more water in the filtrate and results in an increase in urine volume. Because there is less circulating protein, principally albumin, the osmotic pressure of the blood falls. Less osmotic pressure pulling water into the capillaries tips the balance towards hydrostatic pressure, which tends to push it out of the capillaries. The net effect is that water is lost from the circulation to interstitial tissues and cells. This “plumps up” the tissues and cells, a condition termed systemic edema.
Reabsorption and Secretion
The renal corpuscle filters the blood to create a filtrate that differs from blood mainly in the absence of cells and large proteins. From this point to the ends of the collecting ducts, the filtrate or forming urine is undergoing modification through secretion and reabsorption before true urine is produced. Here, some substances are reabsorbed, whereas others are secreted. Note the use of the term “reabsorbed.” All of these substances were “absorbed” in the digestive tract—99 percent of the water and most of the solutes filtered by the nephron must be reabsorbed. Water and substances that are reabsorbed are returned to the circulation by the peritubular and vasa recta capillaries.
Urinalysis
Urinalysis (urine analysis) often provides clues to renal disease. Normally, only traces of protein are found in urine, and when higher amounts are found, damage to the glomeruli is the likely basis. Unusually large quantities of urine may point to diseases like diabetes mellitus or hypothalamic tumors that cause diabetes insipidus. The color of urine is determined mostly by the breakdown products of red blood cell destruction (see Figure 8.8). The “heme” of hemoglobin is converted by the liver into water-soluble forms that can be excreted into the bile and indirectly into the urine. This yellow pigment is urochrome. Urine color may also be affected by certain foods like beets, berries, and fava beans. A kidney stone or a cancer of the urinary system may produce sufficient bleeding to manifest as pink or even bright red urine. Diseases of the liver or obstructions of bile drainage from the liver impart a dark “tea” or “cola” hue to the urine. Dehydration produces darker, concentrated urine that may also possess the slight odor of ammonia. Most of the ammonia produced from protein breakdown is converted into urea by the liver, so ammonia is rarely detected in fresh urine. The strong ammonia odor you may detect in bathrooms or alleys is due to the breakdown of urea into ammonia by bacteria in the environment. About one in five people detect a distinctive odor in their urine after consuming asparagus; other foods such as onions, garlic, and fish can impart their own aromas! These food-caused odors are harmless.
Urine volume varies considerably. The normal range is one to two liters per day. The kidneys must produce a minimum urine volume of about 500 mL/day to rid the body of wastes. Output below this level may be caused by severe dehydration or renal disease and is termed oliguria. The virtual absence of urine production is termed anuria. Excessive urine production is polyuria, which may be due to diabetes mellitus or diabetes insipidus. In diabetes mellitus, blood glucose levels exceed the number of available sodium-glucose transporters in the kidney, and glucose appears in the urine. The osmotic nature of glucose attracts water, leading to its loss in the urine. In the case of diabetes insipidus, insufficient pituitary antidiuretic hormone (ADH) release or insufficient numbers of ADH receptors in the collecting ducts means that too few water channels are inserted into the cell membranes that line the collecting ducts of the kidney. Insufficient numbers of water channels (aquaporins) reduce water absorption, resulting in high volumes of very dilute urine.
Concept Check
- Contrast the following terms: oliguria, anuria and polyuria. What are the differences between these terms as they describe urinary output?
- Explain how urine colour varies based on food consumed and/or hydration levels.
Endocrine Urinary Function
Several hormones have specific, important roles in regulating kidney function. They act to stimulate or inhibit blood flow. Some of these are endocrine, acting from a distance, whereas others are paracrine, acting locally.
Diuretics and Fluid Volume
A diuretic is a compound that increases urine volume. Three familiar drinks contain diuretic compounds: coffee, tea, and alcohol. The caffeine in coffee and tea works by promoting vasodilation in the nephron, which increases GFR. Alcohol increases GFR by inhibiting ADH release from the posterior pituitary, resulting in less water recovery by the collecting duct. In cases of high blood pressure, diuretics may be prescribed to reduce blood volume and, thereby, reduce blood pressure. The most frequently prescribed anti-hypertensive diuretic is hydrochlorothiazide.
Regulation of Nitrogen Wastes
Nitrogen wastes are produced by the breakdown of proteins during normal metabolism. Proteins are broken down into amino acids, which in turn are deaminated by having their nitrogen groups removed. Deamination converts the amino (NH2) groups into ammonia (NH3), ammonium ion (NH4+), urea, or uric acid (Figure 8.9). Ammonia is extremely toxic, so most of it is very rapidly converted into urea in the liver. Human urinary wastes typically contain primarily urea with small amounts of ammonium and very little uric acid.
Watch this video:
Media 8.2. Urinary System, Part 2: Crash Course A&P #39 [Online video]. Copyright 2015 by CrashCourse.
Urinary System Medical Terms not Easily Broken into Word Parts
Urinary System Abbreviations
Many terms and phrases related to the urinary system are abbreviated.
Learn these common abbreviations by expanding the list below.
Diseases and Disorders
Glomerulonephritis
Glomerulonephritis refers to acute or chronic nephritis that involves inflammation of the capillaries of the renal glomeruli. It has various causes, and is noted especially by blood or protein in the urine and by edema. If untreated, it could lead to kidney failure.
Hydronephrosis
Hydronephrosis is a condition whereby the kidneys begin to swell because of the retention of urine. Several conditions can cause hydronephrosis, such as a kidney stone or blood clot. Treatment will vary, depending on the cause (Cleveland Clinic, 2019). To learn more about hydronephrosis the Cleveland Clinic's web page on hydronephrosis.
Polycystic Kidney Disease
Polycystic kidney disease (PKD) is a genetic disease where cysts grow inside the kidneys. The kidneys enlarge from the cystic collections and damage to the filtering structures of the kidneys can occur. As the disease progresses it may lead to chronic kidney disease (American Kidney Fund, 2020). To learn more, visit the Kidney Fund's PKD web page.
Renal Cell Cancer
Renal cell cancer is a cancer occurring in the kidney tubes where urine is produced or collected. This one of the most common cancers found within the kidneys. Removal of the cancerous lesions is the typical approach from a treatment perspective (Centers for Disease Control, 2020). To learn more, visit the CDC web page on Kidney Cancer.
Renal Failure
Renal failure occurs when kidneys suddenly or gradually become unable to filter waste products from blood. When kidneys stop filtering, high level of wastes may build. Two types exist acute kidney failure and chronic kidney failure (Mayo Clinic Staff, 2019a). To learn more about kidney failure visit the Mayo Clinic's page on Chronic Kidney Failure.
Cystitis
Cystitis is inflammation of the urinary bladder, often caused by an infection. A chronic form of this condition is known as interstitial cystitis. Symptoms of cystitis include bladder pressure, voiding frequently, and pain (Mayo Clinic Staff, 2019b). To learn more about cystitis visit the Mayo Clinic's page on Interstitial Cystitis.
Urinary Tract Infection
A urinary tract infection (UTI) is an infection caused by bacteria, or sometimes, fungi. The exact type of bacterial growth is determined by conducting urine for culture and sensitivity (C&S) testing. In rare cases a UTI may be caused by a virus (Lights & Boskey, 2019). For more information, visit Healthline's web page on Urinary Tract Infections.
Urinary Incontinence
Urinary incontinence is a loss of bladder control. Those afflicted with the condition will experience urine leakage from the bladder. Weak bladder muscles are a risk factor for developing this condition (Kim & O'Connell, 2017). To learn more about this condition visit Healthline's webpage Urologic Diseases.
Medical Terms in Context
Medical Specialties and Procedures Related to the Urinary System
Urology is specialty that "addresses the medical and surgical treatment of disorders and diseases of the female urinary tract and the male urogenital system" (Canadian Medical Association, 2018). This specialty focuses on diagnosis, treatment, and surgical repair. Common clinical visits involve kidney stones, kidney failure and bladder dysfunction. To learn more about urology as a specialty visit the Urology Profile (PDF file) authored by the Canadian Medical Association.
Urologist
A urologist is a medical specialist involved in the diagnosis and treatment of urinary and male genitourinary system conditions, disorders, and diseases such as prostate disease, renal and bladder dysfunctions, and others (Canadian Medical Association, 2018).
Procedures and Testing
Urinalysis
A urinalysis is microscopic group of urine testing. This test detects and measures several substances in the urine such as products of normal and abnormal metabolism and bacteria (Lab Tests Online, 2020). To learn more about urinalysis visit Lab Tests Online's Urinalysis web page.
Urine for C&S
Urine for culture and sensitivity. Urine produced by the kidneys is analyzed by way of a urine culture test which can detect and identify bacteria in the urine, which may be causing a urinary tract infection (UTI). If harmful bacteria is found a sensitivity report is generated. This report lists antibiotics sensitive in the treatment of the bacteria present (Lab Tests Online, 2020a). To learn more about Urine for C&S, visit Lab Tests Online's Urine Culture web page.
24 Hour Urine Collection
This is a test whereby all urinary output is collected over a 24-hour period of time. The analysis of urinary output over this extended period of time provides a greater indication of normal or abnormal kidney function (Lab Tests Online, 2017). To learn more a, visit Lab Tests Online's 24-hour Urine Sample article.
CT Scan of Kidney
Computed tomography is a diagnostic imaging procedure that uses a combination of x-rays and computer technology to produce a variety of images. It provides detailed images of the kidney looking for disease, cancer, obstructions and other kidney conditions (Johns Hopkins Medicine, n.d.) . To learn more about a CT scan of the kidney visit Johns Hopkins Medicine's page on Computed Tomography (CT or CAT) Scan of the Kidney.
Cystoscopy
A cystoscopy is a procedure allowing a physician to check for bladder or ureteral problems, such as bladder cancer. An endoscope, also known as a cystoscope, containing a camera at the end of it is used (Canadian Cancer Society, 2020). To learn more about cystoscopy visit the Canadian Cancer Society's Cystoscopy and Ureteroscopy web page .
Dialysis
Dialysis is a treatment that removes waste products from the blood when the kidneys are not fully functioning. This type of therapy is available at home or in a hospital or clinic and there are two main types: peritoneal dialysis and hemodialysis (Kidney Foundation, 2020). To learn more about dialysis visit the Kidney Foundation's Dialysis web page.
Intravenous Pyelogram
An intravenous pyelogram (IVP) is a specialized x-ray designed to produce views of the entire urinary tract. A dye is used to secure the enhanced imaging. The x-rays can also show how well the urinary tract is functioning and any identify any blockages (Canadian Cancer Society, 2020a). To learn more about IVP visit the Canadian Cancer Society's IVP web page.
Kidney Scan
A kidney scan is an imaging test which views the kidneys. It is considered a nuclear imaging test as it uses radioactive tracers to pick up hot or cold spots within the kidney. These variation are are considered abnormal.
Kidney Transplant
When kidneys fail or when a person is in end stage chronic kidney disease, a surgical procedure is performed in the form of a kidney transplant. This procedure involves harvesting a donor kidney which is transplanted into the recipient in need of a functioning kidney to support vital function of the urinary system.
Urinary System Vocabulary
Adventitial
The outermost layer of the wall of a blood vessel.
Apical
Relating to or denoting an apex.
Autonomic
Involuntary or unconscious.
Calyces
A cuplike cavity or structure.
Deamination
The removal of an amino group from a molecule.
Detrusor
A muscle which forms a layer of the wall of the bladder.
Excretion
Waste is eliminated from an organism. In vertebrates this is primarily carried out by the lungs, kidneys and skin.
Homeostasis
A biological process that results in stable equilibrium.
Hydrostatic
Relating to the equilibrium of liquids and the pressure exerted by liquid at rest.
Hypothalmic
A region of the forebrain below the thalamus.
Lethargy
Periods of weakness.
Mitochondria
An organelle found in large numbers in most cells.
Osmosis
A process by which molecules of a solvent tend to pass through a membrane from a less concentrated solution into a more concentrated one.
pH
pH is a measure of how acidic or alkaline a substance is, as determined by the number of free hydrogen ions in the substance.
Prostaglandins
Any of a group of compounds with varying hormone-like effects.
Pseudostratified
Consisting of closely packed cells which appear to be arranged in layers.
Solutes
The minor component in a solution.
Voiding
Excrete (waste matter).
Test Yourself
References
American Kidney Fund. (2020, June 17). Polycystic kidney disease. https://www.kidneyfund.org/kidney-disease/other-kidney-conditions/polycystic-kidney-disease.html
Canadian Medical Association. (2018, August). Urology profile. Canadian Medical Association Speciatly Profiles. https://www.cma.ca/sites/default/files/2019-01/urology-e.pdf
Canadian Cancer Society. (2020). Cystoscopy and ureteroscopy. Canadian Cancer Society: Cancer Information. https://www.cancer.ca/en/cancer-information/diagnosis-and-treatment/tests-and-procedures/cystoscopy/?region=on
Canadian Cancer Society. (2020a). Intravenous pyelogram. Canadian Cancer Society: Cancer Information. https://www.cancer.ca/en/cancer-information/diagnosis-and-treatment/tests-and-procedures/intravenous-pyelogram/?region=on
Centers for Disease Control and Prevention. (2020). Kidney Cancer. https://www.cdc.gov/cancer/kidney/index.htm
Cleveland Clinic. (2019, May 22). Hydronephrosis. https://my.clevelandclinic.org/health/diseases/15417-hydronephrosis
[CrashCourse]. (2015, October 12). Urinary system, part 1: Crash course A&P #38 [Video]. YouTube. https://www.youtube.com/watch?v=l128tW1H5a8
[CrashCourse]. (2015, June 22). Urinary system, part 2: Crash course A&P #39 [Video]. YouTube. https://youtu.be/DlqyyyvTI3k
Johns Hopkins Medicine. (n.d.). Computed tomography (CT or CAT) scan of the kidney. John Hopkins Medicine: Health. https://www.hopkinsmedicine.org/health/treatment-tests-and-therapies/ct-scan-of-the-kidney
Kidney Foundation of Canada. (2020). Dialysis. Kidney Foundation. https://kidney.ca/Kidney-Health/Living-With-Kidney-Failure/Dialysis
Lab Tests Online. (2017, July 10). 24-hour urine sample. https://labtestsonline.org/glossary/urine-24
Lab Tests Online. (2020, June 16). Urinalysis. https://labtestsonline.org/tests/urinalysis
Lab Tests Online. (2020a, January 30). Urine culture. https://labtestsonline.org/tests/urinalysis
Lights, V., & Boskey, E. (2019, March 21). Everything you need to know about urinary tract infection. Healthline. https://www.healthline.com/health/urinary-tract-infection-adults
Mayo Clinic Staff. (2019a, August 15). Chronic kidney disease. Mayo Clinic. https://www.mayoclinic.org/diseases-conditions/chronic-kidney-disease/symptoms-causes/syc-20354521
Mayo Clinic Staff. (2019, September 19). Diabetic nephropathy. Mayo Clinic. https://www.mayoclinic.org/diseases-conditions/diabetic-nephropathy/symptoms-causes/syc-20354556
Mayo Clinic Staff. (2019b, September 14). Interstitial cystitis. Mayo Clinic. https://www.mayoclinic.org/diseases-conditions/interstitial-cystitis/symptoms-causes/syc-20354357
Image Descriptions
Figure 8.2 image description: LeftThe left panel of this figure shows the location of the kidneys in the abdomen. The right panel shows the cross section of the kidney. [Return to Figure 8.2].
Figure 8.5 image description: The left panel of this figure shows the cross section of the bladder and the major parts are labeled. The right panel shows a micrograph of the bladder. [Return to Figure 8.5].
Figure 8.6 image description: Diagrams of the (a) female and (b) male genitalia highlighting the respective urethras. [Return to Figure 8.6].
Figure 8.7 image description: This figure shows the different pressures acting across the glomerulus including blood hydrostatic pressure, blood colloid osmotic pressure, capsular hydrostatic pressure. [Return to Figure 8.7].
Figure 8.8 image description: This color chart shows 8 different shades of yellow and associates each shade with stages of hydration (lightest 3 shades) or dehydration (remaining 5 darker shades). [Return to Figure 8.8].
Unless otherwise indicated, this chapter contains material adapted from Anatomy and Physiology (on OpenStax), by Betts, et al. and is used under a a CC BY 4.0 international license. Download and access this book for free at https://openstax.org/books/anatomy-and-physiology/pages/1-introduction.
tactile corpuscle that responds to light and touch, touch receptor
lamellated corpuscle that responds to vibration
Conservation of the body core heat results in the skin actually freezing
A painful condition in children where bones are misshapen due to a lack of calcium, causing bow leggedness
Specialized cells that produce melanin which is a dark pigment responsible for colouration of skin and hair.
Molecules are transported out of cells. A form of active transport
biological process that results in stable equilibrium
Pertaining to dendrites
abnormal cells in the body dividing uncontrollably.
non cancerous, harmless
Production of cells that can mobilize and establish tumors in other organs of the body
yellow discoloration of the skin
Yellow coloured
abnormal condition of blue (bluish colour, lips and nail beds) caused by deoxygenation.
loss of fluids/water is greater then what is taken in.
pertaining to within the vein
invasion by disease causing organisms
disease causing agents
excision of damaged tissue or foreign object.
collagen-rich skin formed after the process of wound healing that differs from normal skin
formation of a raised or hypertrophic scar
tissue death
pertaining to dermatology
Study of diseases of the skin.
remove by cutting out
